摘要
骨關節炎又稱作退化性關節炎,是一種可動關節衰竭的症狀表現。在關節疾病中,以骨關節炎最為常見,好發於55歲以上的中老年人。骨關節炎的臨床症狀會引起疼痛、僵硬及慢性漸進式的無力感,導致日常的活動不便。如果人類預期壽命增加,骨關節炎將成為最可能發生的問題。因此本文將此疾病提出,供同儕進一步的了解。
關鍵字: 骨關節炎、軟骨退化、疼痛、osteoarthritis、cartilage degenerative、pain
壹、前言
骨關節炎 (osteoarthritis) 又稱作退化性關節炎,是一種可動關節衰竭的症狀表現。主要病徵為關節軟骨退化,由於骨骼之間相互磨擦,而造成劇烈的疼痛1。退化性關節炎被認為與年齡老化有相關,大約有25%的55歲以上中老年人,都有關節疼痛的情形發生。因此對此疾病形成的原因有所了解,可避免惡化之情形繼續發生。
貳、關節軟骨的結構與生化成分2
人類的軟骨是由軟骨細胞及細胞外基質所組成的 (見表一)。軟骨細胞主要控制基質蛋白的合成與遞減,進而影響膠原蛋白與蛋白聚醣的產生。軟骨細胞內含有生長因子,如類胰島素生長因子、表皮生長因子、或纖維生長因子,這些生長因子會促進蛋白聚醣的合成和軟骨細胞的生成。軟骨細胞也含有細胞因子,如白介素 (IL-1) 和腫瘤壞死因子 (TNF-α),這些因子會引起軟骨細胞釋放基質金屬蛋白酶,來抑制膠原蛋白與蛋白聚醣的合成。所以軟骨細胞主要能平衡合成與遞減的功能。膠原蛋白能提供抗張力與阻力。蛋白聚醣是由大量的聚氨基葡萄糖重覆鍵所組成的,每一蛋白聚醣集聚體吸收大量的水分子形成凝膠,具有良好的彈性和膨脹能力,所以能提供抗彈性和壓縮性。
表一 軟骨的生化成分2
水 (Water) (65%-80%) |
軟骨細胞 (Chondrocytes) |
膠原蛋白 (Collagen) |
基質蛋白質 (Matrix proteins) |
玻尿酸分子 (Hyaluronic acid) |
聚氨基葡萄糖 (Glycosaminoglycans /aggrecans) |
蛋白聚糖 (Small proteoglycans) |
參、病理學
可動關節內,軟骨可提供低的摩擦面,使骨頭末端凹凸面間免於受到損害。骨關節炎軟骨的改變,主要發生在軟骨基質內,雖然目前確切的機轉未知,但相信(1)與膠原蛋白的纖維化和蛋白聚醣的釋出分解;(2)軟骨的水合作用增加且變薄;(3)軟骨基質內的分解;(4)基質金屬蛋白酶的釋出,使得關節內的蛋白聚醣和修補能力降低等皆有關2。
隨著年齡增加,軟骨細胞對生長因子的反應下降,細胞因子對軟骨細胞的抑制作用增強,引起細胞因子和生長因子之間比例失調,進而破壞軟骨基質的合成與分解的平衡,造成軟骨進行性的退化。骨關節炎的進展,關節面會變薄,軟骨的軟化,軟骨面的完整性被破壞,纖維化的產生,深層軟骨潰爛,骨頭的延伸皆可能會出現所謂的“骨贅”3。
肆、造成骨關節炎之危險因素
由於全身性和局部性的危險因素的影響,關節有可能發展成骨關節炎 (見圖一)2。隨著年齡的增加,身體的老化,關節軟骨對生長激素的反應變弱,關節日漸磨損,周遭的韌帶變鬆而容易脫臼,關節的穩定度降低。在性別上,尤其停經後的婦女,estrogen的缺乏,骨骼含鈣量的降低,骨骼病變的機會隨之增加,皆會相對增加骨關節炎的發生。此外遺傳因素,家族中有早發性關節退化或多發性關節炎的病史,罹患退化性關節炎的機會也會提高。關節外傷,關節遭遇嚴重的撞擊、拉傷而未徹底的治療,容易引發退化性關節炎。重覆的壓力,如職業性的壓迫,特定種類的運動,屬於機械性關節受損。先天性畸形,關節發育異常而引起關節軟骨的破壞,如膝部的內翻或外翻,下肢不等長,脊椎側彎症。發炎性的關節,像骨折、感染、痛風。肥胖會增加關節面承受的壓力,都是容易引起軟骨的破壞,迫使軟骨提早退化之危險因素4。
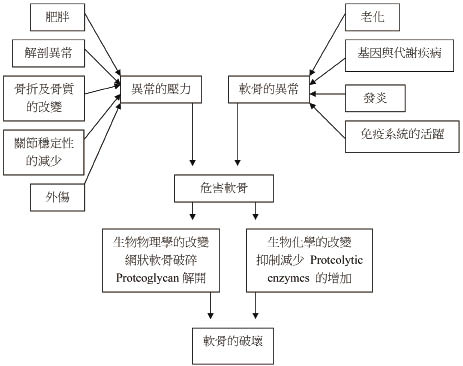
圖一 骨關節炎的危險因素2
伍、臨床表徵與診斷
典型骨關節炎大都發生在中老年人,陳述病患之病痛在膝蓋、臀部、手或脊椎。病患的疼痛和僵硬感最常發生在關節內和關節周圍,一般早晨關節僵硬低於30分鐘,有些關節功能受到限制,造成關節無力感。運動時會有輾紮聲、疼痛,及關節畸形之情形發生5。
骨關節炎症臨床特徵,在關節滑液方面具有高黏度及稍微的白血球增多;在檢驗數值方面,類風濕因子檢測是無反應而紅血球沉降速率、紅血球生化檢查是正常的。在診斷方面,評估病人的病史,關節的臨床檢查及放射線的發現。放射線之發現能證明原發性的骨關節炎,包含關節空間喪失,骨贅的生成,囊腫的形成和下軟骨的硬化6。
陸、治療
骨關節炎的治療包括非藥物治療 (見表二),藥物治療 (見表三)5,7,以及手術處理。
表二 Nonopharmacologic treatment for osteoarthritis 5, 7
Treatment |
Comments |
Exercise |
|
Resistance training Aerobic |
Avoid if joint pain worsens. Progressive training is most effective. Exercises in a pool or partial weight-bearing exercises are often tolerated better than equivalent full-weight-bearing exercises. |
Physical therapy |
Improvement in pain and function (limited data from controlled trials) |
Unloading joint |
|
Cane or crutch |
Improvement in balance and self-confidence, with the cane held on the contralateral side to the affected hip and knee |
Insoles |
Possible reduction in pain and disease progression associated with reducing forces across the joint |
Weight loss |
Recommended on the basis of the recognized association between obesity and osteoarthritis of the knee and hip |
Acupuncture |
Reduces pain on average only moderately after several sessions |
表三 Pharmacologic treatment for osteoarthritis 5,7
Treatment |
Dosage |
Comments |
Acetaminophen |
Up to 1g 4 times a day |
Patients with liver disease or alcoholism should avoid. Prolongs half-life of warfarin |
NSAIDs Naproxen Salsalate Ibuprofen |
375-500 mg twice a day 1500 mg twice a day 600-800 mg 3 to 4 times a day |
Take with food. High rates of gastrointestinal side effects, including ulcers and bleeding. Patients at high risk for gastrointestinal side effects should also take either a proton-pump inhibitor or misoprostol. There is an increased concern about side effects (gastrointestinal or bleeding) when taken with acetylsalicylic acid. Can also cause edema and renal insufficiency. |
Cyclooxygenase-2 inhibitors Celecoxib |
100-200 mg per day |
High doses are associated with an increased risk of myocardial infarction and stroke. Can cause edema and renal insufficiency. |
Glucosamine and Chondroitin |
Glucosamine , up to 1500 mg a day; Chondroitin , up to 1200 mg a day; |
Limited date on efficacy; possible gastrointestinal side effects (e.g., gas, diarrhea); should be taken with food. |
Opiates Tramadol |
50 mg every 6 hr, up to 300 mg a day (immediate release) |
Should reduce dose by 50% in patients with renal insufficiency; may cause flushing, headache, dizziness, insomnia, muscle weakness, and constipation. |
Capsaicin |
0.025-0.075% cream 3 to 4 times a day |
Can irritate mucous membranes. |
Intra-articular injections Hyaluronic acid Steroids |
Varies from 3 to 5 weekly injections, depending on preparation |
Mild to moderate pain at injection site |
一、非藥物治療
物理性的治療,可維持和恢復關節的運動範圍,減輕疼痛和減少肌肉的痙攣,增加肌肉的強度。適當的運動,亦可以增加軟骨中關節滑液的進出,加強關節周圍肌肉、肌腱和韌帶的結構。飲食控制,有效控制體重或減輕體重,減少關節的負荷。有研究指出,體重只要減少5公斤,就可減少50% 的機會發展成症狀性的骨關節炎8。另職能治療,如托板、柺杖、助行器等,目的在減少關節負荷。對於有膝關節內翻的畸形,可利用角度5到10度的腳跟和腳掌軟墊,來矯正生物力學所引起的異常。針灸,在一隨機研究指出,可明顯地減少疼痛和改善生活品質,並且可以維持三個月9。
二、藥物的治療
(一) 非類固醇抗發炎藥物 (nonsteroidal anti-inflammatory drugs)(NSAIDs)、cyclooxygenase-2 (COX-2) inhibitors和acetaminophen
NSAIDs可有效提供骨關節炎症狀的解除,這些藥物具有止痛和抗發炎的特性,但其在胃腸道和腎臟的副作用大。在65歲以上的老年人中,約有30%會因胃潰瘍引起疾病而住院或死亡,皆被認為與NSAIDs的使用有關。對於骨關節炎的治療,於隨機研究顯示NSAIDs和COX-2 inhibitors 是比acetaminophen較有效的治療骨關節炎的疼痛10。由於NSAIDs有較大的毒性,所以acetaminophen仍被建議為第一線的用藥治療。為了降低傳統NSAIDs潛在胃部的毒性副作用,使用COX-2 inhibitors較具專一性來治療,因其對胃黏膜及凝血功能的影響較小,然而最近的試驗結果顯示,COX-2 inhibitors會增加心臟血管的危險,因此限制了它的使用。在一隨機研究顯示,NSAIDs和misoprostol或proton-pump抑制劑合併使用,經內視鏡的檢查後證實,比單獨NSAIDs使用潰瘍數有明顯的降低,且出血的危險降低約82%11。
(二)關節內注射玻尿酸
其主要含有聚胺基葡萄糖多醣複合物,為軟骨基質及滑液的基本成份,具有高黏稠性,可能的機轉為提高關節液黏稠性、抗發炎、維持關節液的恆定性。
(三)關節內注射corticosteroids
當病患在非藥物治療或藥物治療皆無反應時,可於關節內注射corticosteroids來處理。可用於短期的治療,能有效的改善疼痛及增加關節的活動能力,具有局部抗發炎的效果,能明顯減少骨贅的發生。
(四)Glucosamine和Chondroitin Sulfate
葡萄糖胺 (Glucosaminse) 是關節軟骨聚氨基葡萄糖的基本成分,也是合成蛋白聚醣的基本物質。軟骨膠 (chondroitin) 是關節軟骨細胞另一構成要素,具有強力滯留水份作用,提供關節軟骨抗壓縮性的特性。Glucosamine和Chondroitin sulfate廣泛使用在骨關節炎,然而機轉作用尚未清楚。在一些隨機研究顯示12,能減少關節疼痛且較少的副作用。
(五)其它的藥物的治療
鴉片類止痛劑Tramadol用來治療中度至重度疼痛。當病患對NSAIDs有不適的控制治療時,Tramadol可當作輔助治療。 局部止痛劑像番椒晶素 (capsaicin),作用於末梢感覺神經系統能抑制疼痛的感覺,亦能適當地減少疼痛。
三、外科手術
外科手術,一般於在病患有嚴重的骨關節炎,且有持續的疼痛及明顯的功能惡化時才施行。關節鏡清創術 (arthroscopic debridement),移除關節軟骨發炎時引起的碎片物,可以預防關節連接處的阻塞,排除疼痛,預防關節表面快速的磨損。當關節破壞到極致時,唯一治療方式即為全人工膝關節置換術 (totol knee replacement,TKR) 或全人工髖關關節置換術 (totol hip replacement,THR),其置換成效良好,可改善關節變形的矯正,解除疼痛,改善關節功能,進而提升生活品質。
柒、結論
隨著人口的老化,骨關節炎的發生率隨之增加,病因機轉尚清楚,有人認為是機械性的磨損,或腫瘤壞死因子讓軟骨加速被破壞。複雜因子,如遺傳基因、外傷和肥胖互相影響引起這疾病;軟骨細胞四周狀態的改變,也會潛在的引起骨關節炎。所以,骨關節炎大部份發生在原發性骨關節炎,也會藉由其它的病程引起次發性的骨關節炎 (如內分泌、代謝、感染)。骨關節炎的病程從第一次症狀開始到關節的置換可能需要12到18年,或更長的時間13。
因此,此病症之治療目標在於症狀的解除,疼痛的控制,關節的無力感及僵硬感降低,儘量維持關節的可動性和功能性,而達改善病患生活品質之最終目的。
參考資料:
1. Barnes EV, Edwards N L. Treatment of osteoarthritis. South Med J 2005; 98: 205-9.
2. Mandelbaum B, Waddel D. Etiology and pathophysiology of osteoarthritis. Orthopedics. 2005 Feb; 28 (2 Suppl): s207-14.
3. DiCesare PE, Abramson SB. Pathogenesis of osteoarthritis. In: Harris ED, Budd RC, Firestein GS, et al: eds. Kelley's textbook of rheumatology. 7th ed. Vol. 2. Philadelphia: Elsevier/Saunders, 2005: 1493-513.
4. Nevitt MC. Risk factors for knee, hip and hand osteoarthritis. In: Arden N, Cooper C, eds. Osteoarthritis handbook. London: Taylor & Francis, 2006: 23-48.
5. Felson DT . Osteoarthritis of the Knee. N Engl J Med 2006; 354: 841-8.
6. Ruddy S, Harris ED, Sledge CB, Kelley WN. Kelly's Textbook of rheumatology. 6th ed. Philadelphia: Saun 2001: 1410.
7. Lane NE. Osteoarthritis of the Hip. N Engl J Med 2007; 357: 1413-21.
8. Feloson DT, Zhang Y, Anthony JM, et al: Weight loss reduces the risk for symptomatic knee osteoarthriris in women: the Framingham Study. Ann Intern Med 1992; 116: 535-9.
9. Witt CM, Jena S, Brinkhaus B, Liecker B, Wegscheider K, Willich SN. Acupuncture in patients with osteoarthritis of the knee or hip: a randomized, controlled trial with an additional nonrandomized arm. Arthritis Rheum 2006; 54: 3485-93.
10. Felson DT. The verdict favors nonsteroidal antiinflammatory drugs for treatment of osteoarthritis and a plea for more evidence on other treatments. Arthritis Rheum 2001; 44: 1477-80.
11. Lanas A, García-Rodríguez LA, Arroyo MT, et al: Effect of antisecretory drugs and nitrates on the risk of ulcer bleeding associated with nonsteroidal anti-inflammatory drugs, antiplatelet agents, and anticoagulants. Am J Gastroenterol 2007; 102: 507-15.
12. McAlindon TE, LaValley MP, Gulin JP, Felson DT. Glucosamine and chondroitin for treatment of osteoarthritis: a systematic quality assessment and meta-analysis. JAMA 2000; 283: 1469-75.
13. Schurman DJ, Smith RL. Osteoarthritis: current treatment and future prospects for surgical, medical, and biologic intervention. Clinical Orthopaedics& Related Research. 2004; S183-189.
Osteoarthritis Disease and Treatment
Yu-Hui Su 1, Chen-Chun Kuo1 , Yaw-Bin Huang1, Hung-Lung Lin2
Department of Pharmacy, Kaohsiung Medical University Hospital1
Department of Chinese Medicine, Kaohsiung Medical University Hospital2
Abstract
Osteoarthritis (OA), also called degenerative joint disease, is the failure of a diarthrodial joint. Among the joint diseases, OA is the most common form of arthritis, which occurs more frequently in the population of 55 years or old adults. The major clinical symptoms of the OA are pain, stiffness and progressive disability which lead to increasingly limited activities of daily life. If the life expectancy increases, OA will become the major health problem in the future. Thus, this paper presents this disease for further understanding.

