摘要
臨床上常用 warfarin 作為預防心房顫動病人中風的用藥,但 warfarin 不僅與許多藥品、食物產生交互作用,病人也需定期回診抽血檢測 INR (international normalized ratio),造成使用上的不便。2010年10月,美國食品藥物管理局 (Food and Drug Administration, FDA) 核准新型口服抗凝血藥品 dabigatran 為非瓣膜性心房顫動病人中風的預防藥品,替不適合服用 warfarin 或是服用 warfarin 順從性較差的病人提供了另一個方式的選擇。
關鍵字: 心房顫動、中風、dabigatran、warfarin、atrial fibrillation、stroke
壹、前言
根據行政院衛生署的統計,腦血管疾病自民國96年開始列名為國人十大死因的第三名,僅次於惡性腫瘤及心臟疾病;而心房顫動為造成中風的危險因子之一,有心房顫動的病人中風的機率與沒有心血管疾病的人相比,高了將近5倍1。因此,對於心房顫動的治療,除了控制心速及心律之外,預防中風也是另一項重點2。
貳、心房顫動與中風
心房顫動為心臟不正常放電,心房以不協調、雜亂的方式收縮跳動,導致心跳速率、節率異常,為一種常見的心律不整;在臨床上,心房顫動可以透過心電圖來確診,主要臨床表徵為P波消失或不明顯。大部分心房顫動的病人並沒有出現什麼症狀,有些則有心悸、胸悶、胸痛、呼吸急促或暈眩等症狀。
當心房顫動或心房收縮不全時,心臟裡的血液很容易凝集成小血塊。當這些血塊離開心臟隨著血液進入全身循環,便很容易造成缺血性中風 (ischemic stroke) 或全身性栓塞 (systemic embolism),增加病人死亡 (mortality) 或傷殘 (disability) 的機率。根據2010年美國心臟學院 (American College of Cardiology, ACC) 的研究指出,由心房顫動所引起的中風約佔所有中風案例中的15%-20%3,且由心房顫動所引起的中風狀況通常比一般情況來得嚴重。
參、心房顫動的流行病學及治療
造成心房顫動的原因有很多,例如:高血壓、糖尿病、慢性心臟病等。心房顫動也與老化有關;在55歲以下族群中,心房顫動的盛行率僅為0.1%,但在80歲以上的族群中則增加至9%4。一般來說,男性比女性容易得到心房顫動4,但心房顫動的女性病人一旦中風,相對的卻比男性病人來的嚴重並且預後較差1。
心房顫動的治療主要分為兩大目標:穩定血液循環及預防中風。前者可以透過心速控制或心律控制達到目標,例如:服用抗心律不整藥品 class III、class Ia、Ic、β-blocker、calcium channel blocker 及 digitalis;而預防中風主要是採用口服抗凝血藥品,如 warfarin2。
肆、Dabigatran 在治療上的突破
過去幾十年來,用來預防心房顫動引起的中風,幾乎都只能依靠 warfarin。但由於 warfarin 治療濃度區間極為狹窄,因此為了確定使用的劑量,患者需要定期抽血檢驗 INR 以監測凝血時間;同時在接受 warfarin 治療的期間,也需注意食物、藥物與 warfarin 的交互作用,例如:不能食用銀杏或大量深綠色蔬菜等。由於 warfarin 在使用上有許多的限制與不便,常常造成患者服藥順從性 (compliance) 不佳而大幅提高中風的風險,因此,上市安全有效且便利的新型抗凝血製劑已被醫療界熱烈期盼甚久。
於2009年首次發表的 RE-LY,為一全球規模最大的長期臨床隨機試驗,研究內容為評比新型口服抗凝血製劑 dabigatran 與 warfarin 對於預防心房顫動所引起的中風機率的成效。RE-LY 的研究成果發現,每天服用 dabigatran 150 mg BID 或 dabigatran 110 mg BID 與服用 warfarin 相比之下,能減少約1/3及1/5中風及全身性栓塞的風險,同時也能降低2/3顱內出血 (intracranial bleeding) 的風險5,因此預期 dabigatran 將可成為50年來第一個可以取代 warfarin 的藥品。同時,dabigatran 也突破了許多治療上的限制,例如:有可預期的抗凝血作用,因此不需做例行性的凝血功能監測;具有低潛在性的藥物交互作用;與食物無交互作用,所以飲食上亦並無禁忌。
伍、Dabigatran 藥品
一、作用機轉
Dabigatran 是由一種結構與凝血酶抑制劑 α-NAPAP (N-α-(2-naphthylsulfonylglycyl)-4-amidinophenylalanine piperidide) 相似的化合物研發出來的;dabigatran 為 prodrug,其活性代謝物 acyl glucuronides (圖一)6為競爭性的直接凝血酶抑制劑 (direct thrombin inhibitor, DTI),可預防血栓形成,也可防止由凝血酶所激活的血小板聚集現象 (圖二)。
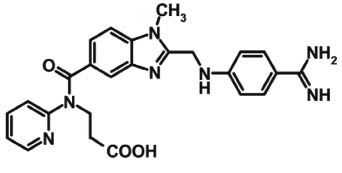
圖一 Dabigatran6
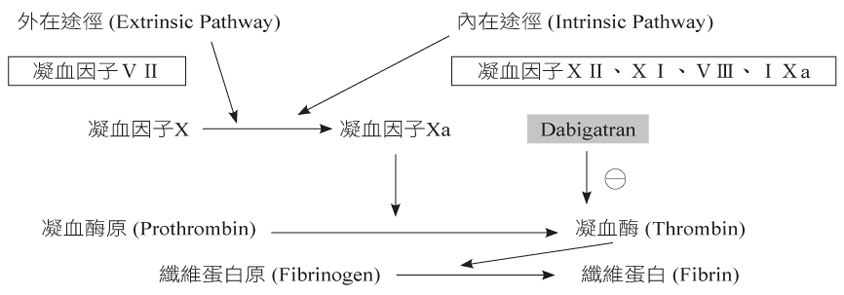
圖二 Dabigatran 於凝血連鎖反應中的角色
二、藥品動力學
(一) 吸收
服藥後1至6小時可達到最高血中藥物濃度,其生體可用率 (bioavailability) 為3%至7%,食物會延遲 dabigatran 在胃腸道的吸收,但對其吸收的程度及生體可用率並沒有影響。
(二) 分布
分布體積 (volume of distribution;Vd) 為50 L至70 L;蛋白結合率 (protein binding) 為35%。
(三) 代謝
在 phase I 透過水解 (hydrolysis) 形成活性代謝物1-O-, 2-O-, 3-O-, 及 4-O-acylglucuronide,進而在 phase II 透過結合 (conjugation) 代謝。
(四) 排泄
主要經由腎臟排泄,排除半衰期 (Elimination Half-Life) 為12至17小時,而腎功能不良的病人則需15至34小時。對於腎功能不良的病人,也可在進行血液透析 (hemodialysis) 後4小時排除68%。
三、劑量及用法
Dabigatran 的劑量取決於病人的腎功能:當病人的 CrCl 大於30 mL/min,建議劑量為150 mg BID;CrCl 介於15 mL/min 至30 mL/min 之間,建議劑量為75 mg BID;CrCl 小於15 mL/min 的病人則不建議使用;可選擇空腹服藥或與食物併服。
四、Dabigatran 的治療效果
大規模長期臨床試驗 RE-LY 一共有18,113位患者參與,分別來自44個國家的964個試驗中心。這些病人同樣患有非瓣膜性心房顫動 (non-valvular atrial fibrillation),且至少有一個中風的危險因子;中風風險評估表 CHADS2 平均得分為2.1;平均年齡為71.5歲;病人被隨機分配到 dabigatran 110 mg BID、150 mg BID 或 adjusted-dose warfarin (INR 2-3);兩組 dabigatran 的試驗為單盲試驗,但 adjusted-dose warfarin 則是 open-labeled;平均追蹤 (follow-up) 的時間為2年,達成率為99.9%。
根據 RE-LY 的研究結果,dabigatran 150 mg BID 比 warfarin 有顯著降低中風或全身性栓塞 (stroke or systemic embolism) 的風險 (p < 0.001)5 (表一)。
表一 Dabigtran 與 warfarin 降低中風機率比較表
Adjusted- dose warfarin |
Dabigatran 110 mg BID |
Dabigatran 150 mg BID |
|
每年中風的機率 (%) |
1.71 |
1.54 |
1.11 |
五、Dabigatran 的不良反應
可分為心肌梗塞 (myocardial infarction) 與出血的危險:兩組不同劑量的 dabigatran 每年增加心肌梗塞的機率均比 warfrin 多了0.2%7;而在出血風險方面,兩組不同劑量的 dabigatran 與 warfarin 相較之下皆能降低總出血 (total bleeding) 與顱內出血的風險;但 dabigatran 150 mg BID 與 warfarin 相較之下卻增加了胃腸道出血 (gastrointestinal bleeding) 的風險8 (表二-三)。
表二 比較 dabigtran 與 warfarin 對於總出血及顱內出血的影響
Adjusted- dose warfarin |
Dabigatran 110 mg BID |
Dabigatran 150 mg BID |
|
所有出血 (%) |
18.23 |
14.66 (p < 0.001) |
16.45 (p = 0.002) |
顱內出血 (%) |
0.76 |
0.23 (p < 0.001) |
0.32 (p < 0.001) |
表三 比較 dabigtran 與 warfarin 對於胃腸道出血的影響
Adjusted- dose warfarin |
Dabigatran 110 mg BID |
Dabigatran 150 mg BID |
|
腸胃道出血 (%) |
1.25 |
1.36 |
1.85 (p < 0.001) |
在所有不良事件 (adverse events) 方面 (圖三)9,兩組劑量的 dabigatran 與 warfarin 皆有相似的結果,但服用 dabigatran 的病人卻有較高比例有消化不良 (dyspepsia) 的現象,這也可能導致病人中斷服藥 (drug discontinuation) 或服藥順從性不佳 (noncompliance)5,9 (表四-五)。
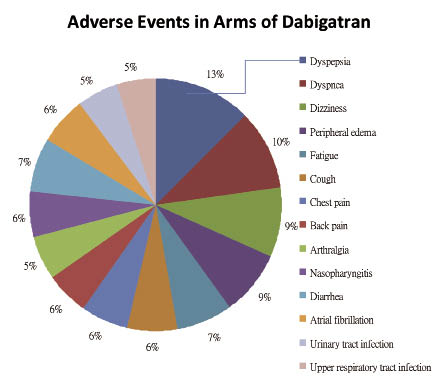
圖三 Dabigatrn 所造成的不良事件9
表四 比較 dabigtran 與 warfarin 造成的消化不良
Adjusted-dose warfarin |
dabigatran 110 mg BID |
dabigatran 150 mg BID |
|
消化不良 (%) |
5.8 |
11.8 (p < 0.001) |
11.3 (p < 0.001) |
表五 服用 dabigtran 的病人有較高中斷服藥的比例 (p<0.001)9
Adjusted-dose warfarin |
dabigatran 110 mg BID |
dabigatran 150 mg BID |
|
一年內中斷服藥的比率 (%) |
10.2 |
14.5 |
15.5 |
兩年內中斷服藥的比率 (%) |
16.6 |
20.7 |
21.2 |
六、懷孕用藥等級
目前並無婦女在懷孕期間服用 dabigatran 造成嬰兒先天性畸形的相關研究,而由製造商進行的動物致畸胎試驗也尚未發表。
陸、結語
美國 FDA 已於2010年10月19日核准 dabigatran 的適應症為非瓣膜性心房顫動病人中風的預防藥品,許多國家如:加拿大、澳洲、日本也已跟進使用,臺灣則在2011年7月核可輸入上市,2012年6月起納入健保給付。
然而,在新藥的使用上,除了需持續觀察臨床上的副作用及不良反應之外,使用專利期內的藥品也須考慮成本效益 (cost-effectiveness) 的問題。雖已有研究指出,在非瓣膜性心房顫動的病人中,年齡大於或等於65歲且 CHADS2 得分大於或等於1分者,選擇 dabigatran 作為中風的預防比 warfarin 較符合成本效益10,但仍須考量使用 dabigatran 的安全性,譬如使用於年齡大於等於75歲的病人有較高顱外出血 (extracranial bleeding) 的風險8、潛在腎功能的累積傷害、缺乏解毒劑及長期使用的監測數據等,因此病人在開始使用 dabigatran 前仍必需做全面性的評估。
參考資料:
1. Wolf PA, Abbott RD, Kannel WB: Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991; 22: 983-8.
2. Prystowsky EN: Management of atrial fibrillation: therapeutic options and clinical decisions. Am J Cardiol 2000; 85: 3D-11D.
3. American College of Cardiology. CardioSmart. Atrial fibrillation. 2010.
4. Go AS, Hylek EM, Phillips KA, et al: Prevalence of diagnosed atrial fibrillation in adults. National implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001; 285: 2370-75.
5. Paikin JS, Haroun MJ, Eikelboom JW: Dabigatran for stroke prevention in atrial fibrillation - the RELY trial. Expert Rev. Cardiovasc. Ther. 9(3), 279-286 (2011).
6. Eisert WG, Hauel N, Stangier J, et al: Dabigatran: An oral novel potent reversible nonpeptide inhibitor of thrombin. Arterioscler Thromb Vasc Biol 2010, 30: 1885-1889.
7. Klein L: Higher-dose dabigatran reduced stroke, but not major hemorrhage, more than warfarin in atrial fibrillation. ACP Journal Club; 152, No.1.
8. Eikelboom JW, Wallentin L, Connolly SJ, et al: Risk of Bleeding With 2 Doses of Dabigatran Compared With Warfarin in Older and Younger Patients With Atrial Fibrillation: An Analysis of the Randomized Evaluation of Long-Term Anticoagulant Therapy (RE-LY) Trial. Circulation 2011; 123: 2363-2372.
9. Connolly SJ, Ezekowitz MD, Yusuf S, et al: Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N Engl J Med 2009; 361: 1139-51.
10. Freeman JV, Zhu RP, Owens DK, et al: Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Intern Med. 2011; 154: 1-11.
A New Anticoagulant — Dabigatran
Wan-Hsuan Lin, Yu-Fang Huang, Wei-Jiin Shou
Department of Pharmacy, National Taiwan University Hospital Hsin-Chu Branch
Abstract
According to the data from Department of Health, Executive Yuan of Taiwan, cerebrovascular disease has been the third of the top ten leading causes of death since 2007, just behind malignant neoplasm and heart disease. As an independent risk factor in stoke, atrial fibrillation (AF) increases the risk of stoke fivefold1. Therefore, the managements of AF include not only restoration and maintenance of sinus rhythm and ventricular rate control but, more importantly, prevention of stroke2. Warfarin is used to prevent stroke in patients with AF. However, it is inconvenient for patients to take warfarin due to poor compliance. For example, they have to be extra careful with drug-drug or food-drug interactions when warfarin is administrated. Besides, regular monitor of international normalized ratio (INR) is required. In October 19, 2010, a novel oral anticoagulant, dabigatran, was approved by the U.S. FDA for preventing stroke in patients with non-valvular AF. The result of The Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) suggests that if patients with AF take dabigatran 150 mg twice daily, the risk of stroke or systemic embolism can be reduced approximately one-third compared to those take adjusted-dose warfarin5. Although dabigatran provides another choice for patients who cannot tolerate side effects of warfarin or are poor compliant, the risk of dabigatran such as bleeding, potential cumulative renal damage or lack of antidote, should still be assessed carefully in long-term use.

