摘要
併用 aspirin 及 P2Y12抑制劑之雙重抗血小板藥是急性冠心症及冠狀動脈支架置放術後預防再次心血管事件之標準治療。Clopidogrel 是目前最常使用的 P2Y12 (purinergic receptor P2Y, G-protein coupled,12) 抑制劑,而新一代 P2Y12血小板抑制劑如 ticagrelor 和 prasugrel,起始作用時間較 clopidogrel 快速,更能抑制血小板活性,進而改善重大心血管事件,但相對而言出血發生率也較高。美國和歐洲心臟學會在最新急性冠心症指引中對 P2Y12抑制劑選用提出建議,與 aspirin 併用雙重抗血小板藥品策略中,ticagrelor 建議用於所有中度至高度缺血性風險患者,而 prasugrel 限用於接受冠狀動脈介入性治療且不曾用過 P2Y12抑制劑之患者。Ticagrelor 和 prasugrel 在冠心症患者預防缺血性事件上可作為 clopidogrel 之有效替代用藥。
關鍵字:急性冠心症、P2Y12抑制劑、ticagrelor、prasugrel
壹、前言
動脈粥樣斑塊 (atherosclerotic plaque) 破裂後,血小板形成血栓 (thrombosis) 覆蓋於受傷的血管壁,會阻塞血管造成組織缺氧和梗塞,進而引起急性心肌梗塞和缺血性中風等血栓性疾病,根據統計民國100年國人十大死因的第二位即是心臟疾病,且世界衛生組織預測西元2020年心血管疾病將成為全球主要死因,因此抑制血栓形成在治療急性冠心症 (acute coronary syndrome, ACS) 和預防後續缺血性併發症相當重要。活化血小板上的腺嘌呤核苷二磷酸 (adenosine diphosphate, ADP) P2Y12受體是引發血小板凝集形成血栓的關鍵步驟,clopidogrel 為最常使用的 P2Y12抑制劑,併用 aspirin 和 clopidogrel 是現今治療急性冠心症及冠狀動脈支架置放術後預防再次心血管事件之標準療法。但受限於 clopidogrel 之藥效作用時間延遲、抑制血小板反應個體變異性大、且具潛在藥物交互作用及不可逆地抑制血小板作用等因素,因此新一代 P2Y12抑制劑持續發展中1,prasugrel 和 ticagrelor 已被美國食品和藥物管理局 (Food and Drug Administration, FDA) 核准,且 ticagrelor 在國內已上市使用。
貳、P2Y12抑制劑
目前抗血小板藥作用於 P2Y12受體可分為兩類:一種為不可逆地與 P2Y12受體結合的 thienopyridine 類藥品如 ticlopidine、clopidogrel 和 prasugrel;另一種為與 P2Y12受體可逆結合的 cyclopentyltriazolopyrimidines 類藥品如 ticagrelor2。
一、 第一代和第二代 thienopyridines 類藥品:ticlopidine 和 clopidogrel
Ticlopidine 是第一個核准的 P2Y12受體抑制劑,但因嗜中性球減少症、血栓性血小板減少性紫斑症 (thrombotic thrombocytopenic purpura) 等副作用,臨床上已很少被用於治療急性冠心症。
Clopidogrel 是前驅藥品,經腸胃道吸收後有85%被酯解酶 (esterase) 水解成無活性代謝物,未水解部分再由肝臟 cytochrome P450 (CYP450) 經二次步驟轉換成活性物才具血小板抑制功能 (圖一)2,因此由吸收至產生抗血小板作用需數小時,且治療反應受 CYP 基因變異影響,特別是 CYP2C19基因多型性會降低其抗凝血功能,若與同為 CYP450代謝之藥品如氫離子幫浦抑制劑 (proton pump inhibitors, PPI) 併用會產生交互作用。Clopidogrel 與 P2Y12受體為不可逆結合,其抑制作用在停藥後會逐漸恢復正常,進行含冠狀動脈繞道手術 (coronary artery bypass grafting surgery, CABG) 手術前建議至少停藥5天3,臨床研究 clopidogrel 可改善急性冠心症和進行緊急或冠狀動脈介入性治療 (percutaneous coronary intervention, PCI) 之病人預後。
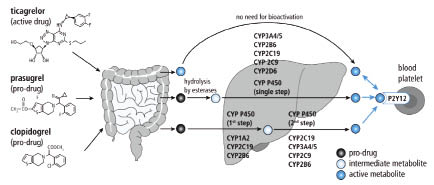
圖一 P2Y12抑制劑之代謝2
二、 第三代 thienopyridines 類藥品:prasugrel (Effient)
Prasugrel 是前驅藥品,主要由 CYP3A4、2B6單一步驟代謝成活性物,起始作用較 clopidogrel 快,且 CYP 基因變異對活性代謝物影響不顯著,個體間變異性低,2-4小時達最大60-70%血小板抑制作用,為不可逆地與 P2Y12受體鍵結抑制血小板活化和凝集 (圖一)2,抑制血小板效果較 clopidogrel 更強。目前 FDA 核准 prasugrel 用於接受 PCI 之急性冠心症患者如不穩定型心絞痛 (unstable angina, UA)、非 ST 段上升型 (non-ST-elevation myocardial infarction, NSTEMI) 或 ST 段上升型心肌梗塞 (ST-elevation myocardial infarction, STEMI) 減少血栓性心血管事件。Prasugrel 停藥後約5天逐漸恢復血小板功能,進行含 CABG 等大手術前至少停藥7天 (表一)3,4。
在納入約13,000名中至高度風險之急性冠心症 (STEMI占26%) 接受 PCI 患者,比較 prasugrel (初始劑量60 mg、維持劑量10 mg qd) 併用 aspirin 與 clopidogrel (初始劑量300 mg、維持劑量75 mg qd) 併用 aspirin 之臨床研究中,觀察兩者預防心血管死亡、非致命性心肌梗塞或非致命性中風之複合事件發生率,追蹤6至15個月,結果發現 prasugrel 比 clopidogrel 減少19%重大心血管事件之相對風險 (9.9% vs. 12.1%, hazard ratio 0.81, p < 0.001),分析資料顯示 prasugrel 在減少非致命性心肌梗塞、進行緊急目標血管修復術和支架栓塞較為顯著8;但 prasugrel 增加嚴重出血 (major bleeding) (2.4% vs. 1.8%, hazard ratio 1.32, p=0.03) 及致命出血 (0.4% vs. 0.1%, p=0.002),在嚴重血小板缺乏發生率二組相同 (0.3%),prasugrel 較少發生中性球缺乏 (neutropenia) (< 0.1% vs. 0.2%, p=0.02);事後次族群分析顯示 prasugrel 對糖尿病病人較有益處,但體重低於60公斤或年紀大於75歲的病人會增加出血風險,且對曾有中風或短暫性腦缺血發作之病人因顯著增加致命性出血和顱內出血故預後較差5。
表一 P2Y12抑制劑特性3,4
藥品 |
Clopidogrel |
Prasugrel |
Ticagrelor |
分類 |
Thienopyridine |
Thienopyridine |
Triazopyrimidine |
前驅藥 |
是 |
是 |
否 |
需經 CYP-450活化 |
是 (二次步驟) |
是 (一次步驟) |
否 |
個體間變異性 |
大 |
小 |
小 |
P2Y12抑制方式 |
不可逆 |
不可逆 |
可逆 |
初始劑量 |
300-600 mg |
60 mg |
180 mg |
維持劑量 |
75 mg qd |
10 mg qd |
90 mg bid |
起始作用* |
2-4小時 |
30分鐘 |
30分鐘 |
達最大抑制作用之時間 |
~12小時† |
2小時 |
2小時 |
平均血小板抑制效力 |
~50% (低) |
~70% (高) |
~95% (高) |
作用時間† |
3-10天 |
5-10天 |
3-4天 |
大手術前需停藥天數 |
5天 |
7天 |
5天 |
*抑制血小板凝集50%;†300 mg 初始劑量
三、 Cyclopentyltriazolopyrimidines 類藥品:ticagrelor (Brilinta)
Ticagrelor 是第一個 cyclopentyltriazolopyrimidine 結構的抗血小板劑,已具藥品活性可直接抑制血小板凝血功能,作用快速,1-3小時達最大血小板抑制作用,且為可逆性抑制 P2Y12受體,半衰期短 (約12小時),停藥後3-5天可恢復血小板止血作用,進行含 CABG 非緊急大手術前至少停藥5天,因快速代謝一天需服藥二次 (表一)3,4,忘記服藥可能增加血栓發生,故需注意服藥順從性。衛生署核准 ticagrelor 用於急性冠心症 (含 UA、NSTEMI 或 STEMI) 患者與 aspirin 併用預防再次栓塞性心血管事件,aspirin 維持劑量應避免每天超過100 mg。Ticagrelor 主要由肝臟 CYP3A4 代謝,禁止與強效 CYP3A4抑制劑 (如 clarithromycin、ketoconazole、atazanavir 和 nefazodone) 等同時使用,亦不建議併用 CYP3A4誘導劑 (如 dexamethasone、rifampicin、carbamazepine、phenytoin 和 phenobarbital),而 PPI 並無明顯影響 ticagrelor 之抗血小板作用6。
在納入約18,000名以介入性或藥品治療之中度至重度急性冠心症 (STEMI 占38%) 患者,比較 ticagrelor (初始劑量180 mg、維持劑量90 mg bid) 併用 aspirin 與 clopidogrel (初始劑量300-600 mg、維持劑量75 mg qd) 併用 aspirin 之臨床研究,觀察兩者預防心血管死亡、心肌梗塞或中風之複合事件發生率,追蹤12個月,結果發現 ticagrelor 比 clopidogrel 降低16%重大心血管事件之相對風險 (9.8% vs.11.7%, hazard ratio 0.84, P < 0.001),進一步分析顯示 ticagrelor 比 clopidogrel 有意義減少心血管疾病死亡、心肌梗塞和支架栓塞,但 ticagrelor 中風發生率較高 (1.5% vs. 1.3%, hazard ratio 1.17, P=0.22);安全性方面,嚴重出血發生率二組相當 (11.6% vs. 11.2%, P=0.43),但 ticagrelor 在與 CABG 無關之出血 (4.5% vs. 3.8%, p=0.03) 和致死性顱內出血 (0.1% vs. 0.01%, p=0.02) 發生率較 clopidogrel 高;ticagrelor 有較多患者發生呼吸困難而停藥 (0.9%) 及心搏徐緩 (4.4%) 等副作用1,7。試驗次族群分析顯示 ticagrelor 併用高維持劑量 aspirin 會減低治療有效性,因此當 ticagrelor 與 aspirin 併用時,FDA 建議 aspirin 維持劑量為75-100 mg2。
參、臨床治療指引應用
美國心臟學院基金會/美國心臟協會 (American college of cardiology foundation/American heart association, ACCF/AHA) 和歐洲心臟學會 (European Society of Cardiology, ESC) 於最新的 ST 段上升心肌梗塞和非 ST 段上升的急性冠心症治療指引中3,8-10,建議口服抗血小板藥品 aspirin 儘快加上 P2Y12抑制劑之雙重藥品治療,ticagrelor 用於所有中度至高度缺血性風險患者,以非侵入性治療之急性冠心症患者應儘快使用 aspirin 加上 P2Y12抑制劑 (clopidogrel 或 ticagrelor) 持續12個月8;而 prasugrel 限用於接受 PCI、未曾用過 P2Y12抑制劑且之前無中風病史及年紀低於75歲患者。對進行緊急 PCI (primary PCI) 的 STEMI 患者和 UA、NSTEMI 接受 PCI 之急性冠心症患者,在 ACCF/AHA 指引中建議 P2Y12抑制劑可選用 clopidogrel 或 ticagrelor 或 prasugrel8,9,UA、NSTEMI 患者應併用 aspirin 至少12個月,接受支架置放患者應併用 aspirin 12個月,與 ticagrelor 同時使用之 aspirin 每日維持劑量為81 mg,而ESC指引對於進行 PCI 之急性冠心症患者,在 P2Y12抑制劑選用上則建議 ticagrelor 或 prasugrel 皆優先於 clopidogrel,除非 ticagrelor 或 prasugrel 不適用,P2Y12抑制劑應儘快加上 aspirin 並持續12個月3,10,除非為出血高風險之病人。STEMI 患者使用緊急血栓溶解劑治療時,可併用 aspirin 和 clopidogrel 至少14天至1年的雙重抗血小板劑作為輔助治療9。
肆、結論
抗血小板劑是治療急性冠心症重要藥物,新藥上市增加用藥選擇性,ticagrelor 具直接抗血小板凝集作用,prasugrel 僅需單一活化步驟,兩者抑制血小板作用比 clopidogrel 迅速且抑制性強,能更有效預防血栓事件,由臨床研究結果 ticagrelor 和 prasugrel 可作為替代 clopidogrel 治療急性冠心症之有效用藥,但 prasugrel 限於接受冠狀動脈介入性治療及無中風病史之患者,所有 P2Y12抑制劑皆不能用於活動性病理性出血患者,ticagrelor 需注意呼吸困難和心搏徐緩等副作用,因此臨床使用上仍需依患者和藥物不同特性選擇最合適之用藥。
參考資料:
1. Damman P. Woudstra P. Kuijt WJ, et al: P2Y12 platelet inhibition in clinical practice. J Throm thrombolysis 2012; 33: 143-153.
2. Sibbing D, Orban M; Massberg S. Potent P2Y12 receptor inhibitors in patients with acute coronary syndrome. Hämostaseologie 2013; 33: 9-15.
3. Hamm CW, Bassand JP, Agewall S, et al: 2011 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2011; 32: 2999-3054.
4. Eshaghian S, Shah PK, Kaul S. Advances in antiplatelet treatment for acute coronary syndromes. Heart 2010; 96(9): 656-61.
5. Wiviott SD, Braunwald E, McCabe CH, et al: Prasugrel versus clopidogrel in patients with acute coronary syndrome. N Engl J Med 2007; 357: 2001-2015.
6. Deeks ED. Ticagrelor: A review of its use in the management of acute coronary syndromes. Drugs 2011; 71(7): 909-933.
7. Wallentin L, Becker RC, Budaj A, et al: Ticagrelor versus clopidogrel in patients with acute coronary syndrome. N Engl J Med 2009; 361: 1045-1057.
8. Jneid H, Anderson JL, Wright RS, et al: 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non-ST-elevation myocardial infarction. Circulation 2012; 126: 875-910.
9. O'Gara PT, Kushner FG, Ascheim DD, et al: 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. Circulation 2013; 127: 529-555.
10. Steg PG, James SK, Atar D, et al: ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012; 33: 2569-2619.
P2Y12 Inhibitors for Acute Coronary Syndrome
Yu-Chuan Tsai, Chien-Hui Chen, Su-Yu Chien
Department of Pharmacy, Changhua Christian Hospital
Abstract
Antiplatelet therapy is the cornerstone of management of acute coronary syndromes (ACS). Dual-antiplatelet therapy of aspirin plus P2Y12 inhibitor is the foundation of treatment to prevent thrombotic complications of ACS and undergoing a coronary stenting procedure. Clopidogel is the most utilized drug that inhibits P2Y12 in platelet. Compared to clopidogrel, the new P2Y12 inhibitors prasugrel and ticagrelor are more potent, more rapid, and more effective in improving major cardiovascular events, with a tendency to increase bleeding. Prasugrel and ticagrelor have been added to updated ACC/AHA and ESC guideline for ACS patients. According to the guidelines, ticagrelor is recommended for all patients at moderate to high risk of ischemic events, and prasugrel is restrictive in P2Y12 inhibitor-naïve patients undergoing PCI. Ticagrelor and prasugrel are effective alternative to clopidogrel for the prevention of ischemic events in ACS patients.

