摘要
大部分文獻顯示肥胖病人使用 vancomycin 較適合使用實際體重建議劑量,然而目前也有文獻建議較低的每日劑量仍可達到有效治療濃度並降低腎毒性,因此本文運用藥物血中濃度監測 (Therapeutic Drug Monitoring,TDM) 結果, 回溯性蒐集某醫學中心99年1月至102年4月使用 vancomycin,腎功能正常,年齡介於18歲至65歲非老年人,依據 BMI 指數區分為正常體重 (18.5 ≦ BMI < 24 kg/m2) 和肥胖 (BMI ≧ 27 kg/m2) 兩大族群,並依據當時監測結果算出藥物動力學參數,比較兩者之間分佈體積和清除率之差異,以利進一步分析肥胖病人適當的建議劑量。
初步結果肥胖病人共蒐集49位,正常體重病人53位,肥胖病人平均每日使用劑量以理想體重表示為32.6 ± 8.35 mg/kg/day IBW,正常體重病人為30.37 ± 8.44 mg/kg/day IBW;給藥間隔肥胖病人為9.92 ± 2.61 hr,正常體重病人為10.38 ± 2.45 hr,兩者並無統計上差異,然而 TDM 監測結果肥胖病人平均 vancomycin 波峰濃度為21.4 ± 7.11 μg/mL,正常體重病人為25.43 ± 8.9 μg/mL;波谷濃度肥胖病人為8.44 ± 3.98 μg/mL,正常體重病人為10.9 ± 5.81 μg/mL,兩者均較正常體重病人為低,並具有統計上差異 (p < 0.05),進一步分析藥物動力學參數,發現肥胖病人平均分佈體積為48.42 ± 14.26 L,高於正常體重病人42.46 ± 11.73 L;清除率肥胖病人平均為5.99 ± 2.0 L/h,高於正常體重病人4.67 ± 1.79 L/h,兩者均具有統計上差異 (P < 0.05),且發現肥胖病人 vancomycin 清除率和調整體重的相關性優於和實際體重的相關性 (r = 0.4431 vs 0.3524,P < 0.05),此結果暗示著非老年肥胖病人較適合使用調整體重建議劑量。
關鍵字: vancomycin、藥物血中濃度監測、藥物動力學
壹、前言
Vancomycin 主要用於革蘭氏陽性菌感染尤其是針對 methicillin-resistant staphylococcus aureus (MRSA) 引起的感染,在2009年美國感染相關協會針對 vancomycin 提出建議,建議 vancomycin 波谷濃度應由原來5-15 μg/mL 提升至10-20 μg/mL 以避免產生抗藥性,並建議在腎功能正常的病人使用 vancomycin 的建議劑量為15-20 mg/kg Q8H-Q12H1,而目前針對肥胖病人,因分佈體積和清除率的增加,大部分文獻顯示應使用實際體重建議劑量會比使用理想體重來的恰當2-4,而早期研究更是發現年輕的肥胖病人,因有較高清除率,因此需要較高劑量才能達適當的波谷濃度範圍2,3,然而近年 Lodise TP 等人研究發現,病人體重101公斤以上,或是使用高劑量 vancomycin (≧ 4g/day),是較容易產生腎毒性5,6,因而臨床上大家對於肥胖病人使用實際體重建議劑量仍存有一些疑慮,免不了擔心如此高劑量是否會引起腎毒性,而在2012年 Reynolds DC 等人針對年齡18歲以上,腎功能正常的肥胖病人研究顯示,肥胖病人分別使用實際體重建議劑量 (30-45 mg/kg/day) 和經由修改較低的每日劑量15-20 mg/kg/day相比,較低劑量仍可達到有效治療濃度並降低腎毒性7,因此本研究針對腎功能正常之非老年人探討,藉由某醫學中心 vancomycin 藥物血中濃度監測 (therapeutic Drug monitoring,TDM) 結果,回溯性分析肥胖和正常體重之病人,探討藥物動力學參數 (pharmacokinetic parameters) 是否有改變,以求適當的建議劑量。
貳、研究方法
利用某醫學中心之 TDM 資料庫,回溯性蒐集99年1月至102年4月使用 vancomycin,腎功能正常,年齡介於18歲至65歲之間之非老年人 (排除加護病房病人),並依據 BMI 指數 (表一) 區分為正常體重和肥胖兩大族群,所有病人接受間歇性 (intermittent) 投藥方式 (QD 或 Q12H、Q8H、Q6H) 給予 vancomycin,且經由靜脈輸注給藥,在第一次達血中穩定狀態 (steady-state) 進行 TDM 監測,依據當時監測結果以波峰濃度 (peak concentration)、波谷濃度 (trough concentration) 算出藥物動力學參數9,比較兩者之間分佈體積、清除率之差異性,以利進一步分析肥胖病人適當的建議劑量。
參、肥胖定義與統計分析
一、肥胖定義8
根據行政院衛生署 (現更名衛生福利部) 公佈國人成人肥胖為身體質量數 (body mass index;BMI) 超過27 kg/m2;正常體重為 BMI 值介於18.5至24.0 kg/m2之間 (表一),(BMI 值為體重除以身高的平方)。
表一 成人肥胖定義8
|
身體質量指數 (BMI)(kg/m2) |
體重過輕 |
BMI < 18.5 |
正常範圍 |
18.5 ≦ BMI < 24 |
異常範圍 |
過重:24 ≦ BMI < 27 輕度肥胖:27 ≦ BMI < 30 中度肥胖:30 ≦ BMI < 35 重度肥胖:BMI ≧ 35 |
二、統計分析
運用電腦 EXCEL 程式使用 student's t-test 和線性迴歸 (linear regression) 做為統計之方法,以P < 0.05視為有意義之差異。
肆、結果
根據某醫學中心 TDM 資料庫,回溯性蒐集99年1月至102年4月使用 vancomycin 之肥胖病人共49位,正常體重病人53位,病人基本資料如表二,肥胖病人平均每日使用劑量以理想體重表示為32.6 ± 8.35 mg/kg/day IBW,正常體重病人為30.37 ± 8.44 mg/kg/day IBW;給藥間隔肥胖病人為9.92 ± 2.61 hr,正常體重病人為10.38 ± 2.45 hr,兩者並無統計上差異,然而 TDM 監測結果肥胖病人平均 vancomycin 波峰濃度為21.4 ± 7.11 μg/mL,正常體重病人為25.43 ± 8.9 μg/mL;波谷濃度肥胖病人為8.44 ± 3.98 μg/mL,正常體重病人為10.9 ± 5.81 μg/mL,兩者均較正常體重病人為低,並具有統計上差異 (p < 0.05)(表三),進一步分析藥物動力學參數,發現肥胖病人平均分佈體積為48.42 ± 14.26 L,高於正常體重病人42.46 ± 11.73 L;清除率肥胖病人為5.99 ± 2.0 L/h,高於正常體重病人4.67 ± 1.79 L/h,兩者均具有統計上差異 (P < 0.05)(表四),且發現肥胖病人 vancomycin 清除率和調整體重的相關性優於和實際體重的相關性 (r = 0.4431 vs 0.3524,P < 0.05)(圖一)。
表二 肥胖和正常體重病人基本資料
|
正常體重 (N=53 ) |
肥胖 (N=49) |
P value |
年齡 (歲) |
47.26 ± 12.01 |
46.49 ± 11.8 |
0.744 |
男性 |
37 |
35 |
|
女性 |
16 |
14 |
0.858 |
身高 (公分) |
165 ± 7.39 |
166 ± 8.78 |
0.394 |
實際體重 (公斤) |
59.37 ± 7.14 |
86.29 ±14.30 |
< 0.0001* |
調整體重 (公斤) |
59.74 ± 7.30 |
71.30 ± 10.33 |
< 0.0001* |
理想體重 (公斤) |
59.99 ± 8.00 |
61.31 ± 9.37 |
0.476 |
BMI (kg/m2) |
21.74 ± 1.52 |
31.03 ± 3.68 |
< 0.0001* |
Scr (mg/dL) |
0.88 ± 0.18 |
0.93 ± 0.19 |
0.111 |
註:1.* student's t-test,P < 0.05視為有意義之差異;性別:chi-square
2. 調整體重=理想體重 + 0.4 × (實際體重-理想體重)9
3. 數據格式 平均值±標準差
表三 肥胖和正常體重病人 vancomycin 濃度比較
|
正常體重 (N=53 ) |
肥胖 (N=49) |
P value |
劑量 (mg/kg/day IBW) |
30.37 ± 8.44 |
32.6 ± 8.35 |
0.182 |
給藥間隔 (h) |
10.38 ± 2.45 |
9.92 ± 2.61 |
0.400 |
波峰濃度 (μg/mL) |
25.43 ± 8.9 |
21.4 ± 7.11 |
0.0135* |
波谷濃度 (μg/mL) |
10.9 ± 5.81 |
8.44 ± 3.98 |
0.0138* |
註:* student's t-test,P < 0.05視為有意義之差異
表四 肥胖和正常體重病人 vancomycin 藥物動力學參數比較
|
正常體重 (N=53 ) |
肥胖 (N=49) |
P value |
排除速率常數 (h-1) |
0.11 ± 0.039 |
0.13 ± 0.036 |
0.0265* |
分佈體積 (L) |
42.46 ± 11.73 |
48.42 ± 14.26 |
0.0229* |
清除率 (L/h) |
4.67 ± 1.79 |
5.99 ± 2.0 |
0.0006* |
清除率 (mL/min) |
77.77 ± 29.86 |
99.8 ± 33.09 |
0.0006* |
半衰期 (h) |
6.89 ± 2.51 |
5.74 ± 1.56 |
0.0067* |
註:* student's t-test,P < 0.05視為有意義之差異
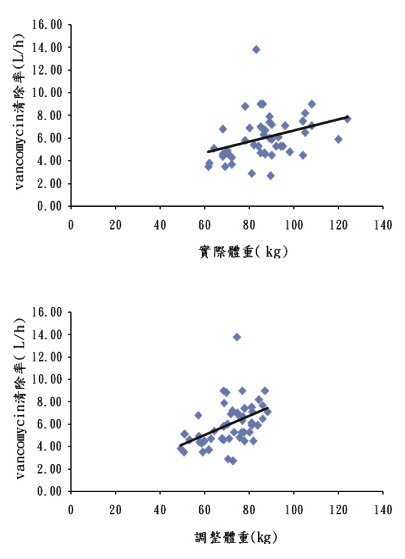
圖一 肥胖病人 vancomycin 清除率和調整體重、實際體重之相關性 (r=0.4431 vs 0.3524,P < 0.05)
伍、討論
本研究針對非老年人,經由回溯性蒐集,發現肥胖病人平均每日使用劑量以理想體重表示為32.6 ± 8.35 mg/kg/day IBW,正常體重病人為30.37 ± 8.44 mg/kg/day IBW;給藥間隔肥胖病人為9.92 ± 2.61 hr,正常體重病人為10.38 ± 2.45 hr,兩者並無統計上差異,然而 TDM 監測結果顯示肥胖病人 vancomycin 波峰、波谷濃度均低於正常體重病人,並具有統計上差異 (p < 0.05)(表三),尤其肥胖病人波谷濃度8.44 ± 3.98 μg/mL低於正常濃度範圍 (波谷正常濃度範圍:10-20 μg/mL)1,這結果或許是因分佈體積和清除率增加而導致濃度降低 (表四),Blouin RA 等人和 Bauer L.A. 等人的研究也同樣針對非老年肥胖病人,研究中指出這些病人有較高的清除率,因此要使用較高劑量,以達適當的波谷濃度2,3,而一般針對肥胖病人建議劑量,目前仍有許多不同看法,有學者建議肥胖病人使用 vancomycin,建議負載劑量 (loading dose) 應使用實際體重計算,而維持劑量 (maintenance dose) 應使用肌酸酐清除率 (creatine clearance; CLcr) 來預估藥物的清除率,再進一步算出適當劑量10,而一臨床上在評估肌酸酐清除率過程中,往往會面臨若使用實際體重有可能會高估病人清除率,使用理想體重有可能會低估病人清除率11,12,而2011年 Leong JV 等人研究顯示,在肥胖病人使用調整體重來計算肌酸酐清除率,進而估算 vancomycin 清除率,會比用實際體重來的好,並認為應使用調整體重計算 vancomycin 劑量13,而這和我們的研究結果有些許的相似,我們研究結果顯示 vancomycin 清除率和調整體重的相關性優於和實際體重的相關性,並具有統計上差異 (r = 0.4431 vs 0.3524,P < 0.05)(圖一),因此在非老年人或許較適合使用調整體重建議劑量,如此一來較可解決使用理想體重建議劑量而導致濃度偏低,進而影響療效,而使用實際體重建議劑量又可能會面臨高劑量易產生腎毒性的風險。
陸、結論
此結果顯示非老年肥胖病人若是使用理想體重建議劑量,可能會導致濃度偏低,進而影響療效;此外肥胖病人 vancomycin 清除率和調整體重的相關性優於和實際體重的相關性,也暗示著非老年肥胖病人較適合使用調整體重建議劑量,然而這仍需要有更多的案例加以佐證,以提供肥胖病人最適當的建議劑量。
Vancomycin Pharmacokinetics in Obese Patients
Chun-Lan Yeh, Hui-Chen Su, Hue-Yu Wang
Department of Pharmacy, Chi Mei Medical Center
Abstract
The aim of this study was to determine an appropriate dose of vancomycin for non-elderly obese patients in Taiwan.
This is a retrospective study conducted at a medical center which has pharmacist-guided therapeutic drug monitoring programs. Patients with normal renal function and age 18 to 65 years who received vancomycin between Jan 1, 2010 to April 30, 2013 were recruited and divided into two groups, obese subjects (BMI ≧ 27 kg/m2) and normal weight control (18.5 ≦ BMI < 24 kg/m2). Pharmacokinetic parameters alteration were computed to compare the difference of volume of distribution (Vd)、clearance (CL) between obese and normal weight patients, and to determine the appropriate vancomycin dose.
There were no significant differences between two groups in the interval and dosage of vancomycin (means of dosage were respectively 32.6 ± 8.35 mg/kg/day IBW in the obese patients and 30.37 ± 8.44 mg/kg/day IBW in the normal weight patients), but the peak and trough concentration were significantly lower in the obese patients than those in the normal weight patients. Further analysis of pharmacokinetic parameters, the mean Vd and CL in the obese patients were much significantl than those in the normal weight patients. The clearance of vancomycin in obese patients have a better correlation with adjusted body weight (ABW) than total body weight (TBW) (r = 0.4431 vs 0.3524,P < 0.05). These results implied that ABW should be used to calculate vancomycin doses for non-elderly obese patients.
參考資料:
1. Rybak M, Lomaestro B, Rotschafer JC, et al: Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm 2009 Jan 1; 66(1): 82-98.
2. Blouin R <A, Bauer LA, Miller DD, et al: Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother 1982; 21: 575-80.
3. Bauer LA, Black DJ, Lill JS.: Vancomycin dosing in morbidly obese patients. Eur J Clin Pharmacol 1998; 54: 621-5.
4. Vance-Bryan K, Guay DR, Gilliland SS, et al: Effect of obesity on vancomycin pharmacokinetic parameters as determined by using a Bayesian forecasting technique. Antimicrob Agents Chemother 1993; 37: 436-40.
5. Lodise TP, Patel N, Lomaestro BM, et al: Relationship between initial vancomycin concentration-time profile and nephrotoxicity among hospitalized patients. Clin Infect Dis 2009; 49: 507-14.
6. Lodise TP, Lomaestro B, Graves J, et al: Larger vancomycin doses (at least four grams per day) are associated with an increased incidence of nephrotoxicity. Antimicrob Agents Chemother 2008; 52: 1330-36.
7. Reynolds DC, Waite LH, Alexander DP, et al: Performance of a vancomycin dosage regimen developed for obese patients. Am J Health Syst Pharm 2012; 69: 944-50.
8. 衛生福利部www.mohw.gov.tw
9. Winter ME: Basic Clinical Pharmacokinetics, 5th ed. Philadelphia, Lippincott Williams & Wilkins, 2010: 459-87.
10. Janson B, Thursky K.: Dosing of antibiotics in obesity. Curr Opin Infect Dis 2012; 25: 634-49.
11. Spinler SA, Nawarskas JJ, Boyce EG, et al: Predictive performance of ten equations for estimating creatinine clearance in cardiac patients. Ann Pharmacother 1998; 32: 1275-83.
12. Dionne RE, Bauer LA, Gibson GA, et al: Estimating creatinine clearance in morbidly obese patients. Am J Hosp Pharm 1981; 38: 841-44.
13. Leong JV, Boro MS, Winter M.: Determining Vancomycin Clearance in an Overweight and Obese Population. Am J Health Syst Pharm 2011; 68: 599-603.

