摘要
注意力不足/過動症 (Attention Deficit/Hyperactivity Disorder, ADHD) 的治療可分為藥物治療、行為治療與藥物治療合併行為治療三大類;美國國立衛生研究院 (National Institutes of Health, NIH) 於 ADHD 治療指引指出,藥物治療合併行為治療與單獨使用藥物治療控制 ADHD 症狀的效果相當,且遠優於行為治療;藥物治療合併行為治療對於非 ADHD 核心症狀的改善則有更佳的效果。
目前國內核准的 ADHD 治療藥物有 methylphenidate (MPH) 與 atomoxetine 兩種,其中 methylphenidate 在藥理分類上屬於精神興奮劑 (psychostimulants),是國內外治療兒童 ADHD 的主要藥物,因其作用時間僅約4小時,故劑型上又可分為一般劑型 (IR-MPH) 與長效劑型 (ER-MPH) 兩種。
口服圓粒藥物吸收系統 (Spheroidal Oral Drug Absorption System;SODAS) 是由 Elan 公司所研發之多重顆粒 (multiparticulate technology) 技術,其中包含了速效型 (immediate release) 與持續釋放型顆粒 (sustained release);速效型顆粒具有快速作用的效果,持續釋放型顆粒則可在服用藥物經過特定的時間之後再將藥物釋放出來,達到與服用2次藥物相近的血中藥物濃度曲線。
ER-MPH 不同的緩釋技術,呈現不同的藥物動力學特性與療效;並沒有一個 ER-MPH 製劑的療效明顯地優於其它製劑,選擇 ER-MPH 製劑最重要的考量應該是以各種患者治療需求為出發點,為病人選擇最適合的製劑。
關鍵字: 注意力不足/過動症、口服圓粒藥物吸收系統、methylphenidate、精神興奮劑、psychostimulants
壹、前言
藥物治療為控制 ADHD 核心症狀最快速、有效的治療方法;在美國 (1990-1993),90%的 ADHD 青少年及兒童患者使用的藥物為精神興奮劑,而其中使用量最大的藥物 (佔全部精神興奮劑的71%) 即為 MPH1,亦為國內目前唯一被核准使用於治療 ADHD 之精神興奮劑藥物。
雖說 MPH 控制 ADHD 核心症狀的效果顯著,但實際上 ADHD 孩童的服藥遵囑性卻只有56%-75%;Pappadopulos 等人的研究發現,雖然89.8%的家長認為孩童有完全依照醫師指示服用 IR-MPH,但藉由唾液樣品檢驗後,實際上有依照醫師指示服用的孩童只佔全部的53.5%,將近1/4 (24.5%) 的患者的唾液樣品顯示孩童並未依照醫師指示服藥2,因此 ADHD 的治療除了要克服就診率、用藥意願的問題外,還需要克服孩童的遵囑性問題。OROS (osmotic-controlled release oral delivery system,滲透泵型控釋系統) 技術設計的 OROS MPH 則可以克服一天多次的給藥模式所造成的 ADHD 患童服藥順從性不佳的問題。
另 Thompson 等人於2006年的研究報告卻顯示約有32%的患者無法由 IR-MPH 轉換為 OROS MPH,其主要原因推測是 OROS MPH 與 IR MPH 間之劑量轉換的問題,且轉換失敗主因為缺乏療效3。Gormez 等人於2013年針對以 OROS MPH 取代 IR-MPH 的研究報告更指出,約有43%服用 OROS MPH 的患者需要另外補充 IR-MPH 方可達到理想的治療效果;在需要另外補充 IR-MPH 的受試中,75%的患者需要在傍晚另行補充 IR-MPH,12.5%的患者需要於上午另行補充 IR-MPH,其餘12.5%的患者則在上午及下午都需要補充 IR-MPH4,方可達到與原先使用 IR-MPH 相近的療效。
造成 OROS MPH 劑量轉換或療效不佳問題的主因是 OROS MPH 之速效劑量僅有全部劑量的22%;以原本每日服用3次 IR-MPH 10 mg 的患者來說,轉換每日早上服用一次 OROS MPH 36 mg 後,OROS MPH 在早上釋放出來的 MPH 實際上只有8 mg,很容易因為劑量不足造成起始作用速度過慢或療效不佳。但也因為 OROS MPH 採取的是“階梯式上升型”的藥物血中濃度變化的設計,減少了 MPH 濃度在患者體內的變化,也可減少因血中 MPH 濃度劇烈變化而造成的不適感 (副作用)5。
貳、作用機轉
一、SODAS 劑型簡介
口服圓粒藥物吸收系統 (Spheroidal Oral Drug Absorption System;SODAS) 是由 Elan 公司所研發之多重顆粒 (multiparticulate technology) 技術,其中包含了速效型 (immediate release) 與持續釋放型顆粒 (sustained release);速效型顆粒具有快速作用的效果,持續釋放型顆粒則可在服用藥物經過特定的時間之後再將藥物釋放出來,達到與服用2次藥物相近的血中藥物濃度曲線6。
目前採用 SODAS 劑型並經過美國 FDA 核准上市的藥品除了 Ritalin LA 外,尚有 Avinza (morphine)、Luvox CR (fluvoxamine) 與 Focalin XR (dexmethylphenidate) 等。
Ritalin LA 每個膠囊所充填的圓粒中,50%的劑量為快速釋放的圓粒,50%劑量為腸溶包衣的延遲釋放圓粒 (圖一),因此能在服用後快速釋放 methylphenidate 達到快速作用的效果;延遲釋放圓粒在服用後大約4個小時會接著釋出 methylphenidate7-9。
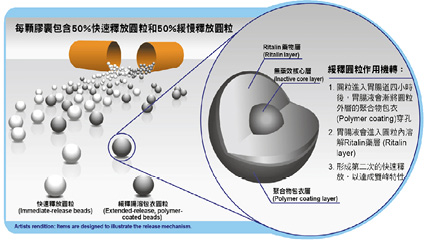
圖一 SODAS 劑型之 Methylphenidate 製劑 (Ritalin LA)
Ritalin LA 的主成份為 methylα-phenyl-2-piperidineacetate hydrochloride,結構式為 (圖二)。
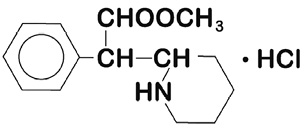
圖二 Methylphenidate 之化學結構 (MW:269.77)8
二、藥理機制
Ritalin LA 持續性藥效膠囊的主成份 methylphenidate hydrochloride,對於 ADHD 的治療作用模式未明,但 methylphenidate 被認為是阻斷 norepinephrine 和多巴胺的再吸收進入突觸前神經元,而增加了這些 monoamines 於神經元外空間的釋出。Methylphenidate 是由 d-threo 式和 l-threo 式旋光物組成的消旋混合物,d-threo 式旋光物的藥理活性大於l-threo 式旋光物8。
參、藥物動力學
一、吸收
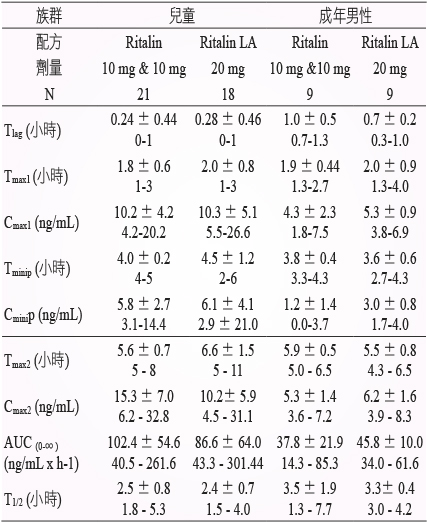
口服 Ritalin LA 持續性藥效膠囊後,會產生雙峯 (bi-modal) 的血漿濃度-時間圖。Ritalin LA 持續性藥效膠囊最初的吸收速率和 Ritalin 錠劑類似,二種劑型的吸收速率參數值相近。Ritalin LA 持續性藥效膠囊一天給藥一次,或給與 Ritalin 錠劑兩次,兩個劑量給藥間隔4小時,二者在兩個濃度高峯間藥品濃度降到最低的時間 (Tminip),和到達第二個最高血中濃度的時間 (Tmax2) 類似,兩個濃度高峯間隔時間均為4小時 (圖三及表一)。
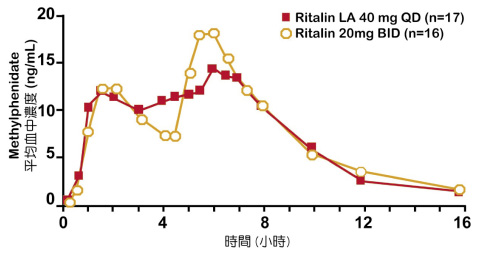
圖三 單劑給與 Ritalin LA 持續性藥效膠囊40毫克和間隔4小時給與兩劑 Ritalin 錠劑後的 methylphenidate 平均血漿濃度-時間圖8
表一 單劑給與 Ritalin LA 持續性藥效膠囊20毫克和間隔4小時給與兩劑 Ritalin 錠劑後的平均值 ± 標準差及藥物動力學參數範圍7,8
二、分佈
Methylphenidate 與血漿蛋白的結合率很低 (10-33%),d-methylphenidate 的分佈體積為2.65 ± 1.11 L/kg,l-methylphenidate 的分佈體積為1.80 ± 0.91 L/kg8。
三、代謝
在兒童的 methylphenidate 口服絕對生體可用率,d-methylphenidate 為22 ± 8%,l-methylphenidate 為5 ± 3%,顯示大部份的藥品在進入全身性吸收前就被代謝。Methylphenidate 藉由 Carboxylesterase CES1A1 進行快速的生物轉換,且大部份產生去酯化代謝物 alpha-phenyl-2-piperidine acetic acid (ritalinic acid),在血漿中只能檢測到少量的氫氧化代謝物 (如 hydroxymethylphenidate 與 hydroxyritalinic acid)。治療活性主要來自於原型藥7,8。
四、排除
一天一次重覆投與 Ritalin LA 持續性藥效膠囊。Ritalinic acid 的半衰期約為3-4小時。d-methylphenidate 全身清除率約0.4 ± 0.12 L/h/kg;l-methylphenidate 約為0.73 ± 0.28 L/h/kg。口服投與 methylphenidate 的速放劑型後48-96小時內,78-97%的劑量以代謝物的型態由尿液排出,1-3%由糞便排出。只有少量 (< 1%) 未代謝之 methylphenidate 在尿中出現。大部份的劑量以 ritalinic acid 的形式 (60-86%) 由尿液排出7,8。
肆、療效
一、 隨機、雙盲、安慰劑對照、平行試驗設計的臨床試驗7, 8
一項隨機、雙盲、安慰劑對照、平行試驗設計的臨床試驗評估 Ritalin LA (methylphenidate hydrochloride) 持續性藥效膠囊,對象為134名6至12歲依據 DSM-IV 診斷為 ADHD 的兒童,每日早上給與 Ritalin LA 一劑,每日劑量10-40 毫克,或給與安慰劑,治療達2 週。病人的學校班導師需在基值期及每週填寫 Conners ADHD/DSM-IV 量表的教師分量表 (CADS-T)。以 CADS-T 量表用來評估過動和注意力缺乏的症狀,分析由基值至治療最後一週的 CADS-T 分數改變,作為主要療效評估的數據。以 Ritalin LA 治療的病人,相較於以安慰劑治療的病人,症狀分數自基值的改變,有顯著的改善,且具統計意義 (圖四)。
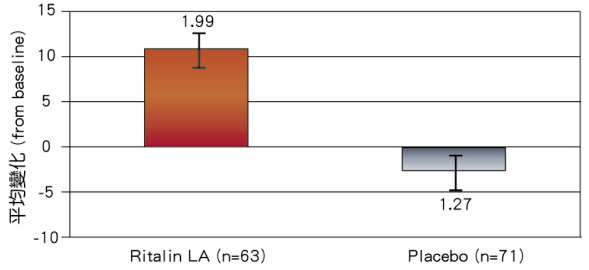
圖四 CADS-T 分量表-與基值比較分數改變的平均值7,8
*誤差線 (error bar) 代表平均標準差
二、 隨機、單盲、安慰劑對照、交叉實驗設計的臨床試驗10
一項隨機、單盲、安慰劑對照、交叉實驗設計的多試驗中心擬課堂臨床試驗,比較 Ritalin LA 20 mg、OROS MPH 18 mg、36 mg 與安慰劑改善 ADHD 核心症狀效果及數學表現的差異。對象為36名6至12歲依據 DSM-IV 診斷為 ADHD 的兒童。試驗結果顯示,在給予藥物0-8小時間,Ritalin LA 20 mg 改善注意力 (SKAMP-attention,圖五)、行為舉止 (SKAMP-deportment,圖六) 與綜合 (SKAMP-combine,圖七) 分數的效果顯著優於OROS MPH 36 mg、18 mg 與安慰劑;使用 Ritalin LA 20 mg 的兒童之數學答題數 (圖八) 與正確數 (圖九) 也優於 OROS MPH 36 mg、18 mg 與安慰劑。
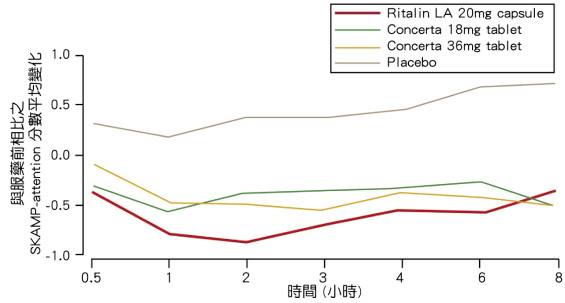
圖五 Ritalin LA 20 mg 與 OROS MPH 18 mg、36 mg 改善注意力效果 (SKAMP-attention) 改善率比較圖10
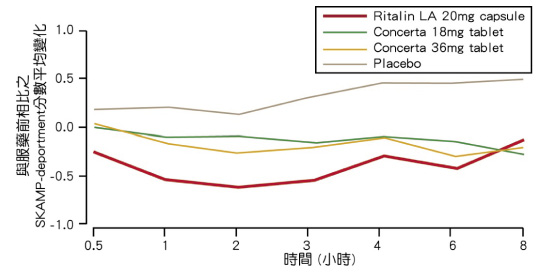
圖六 Ritalin LA 20 mg 與 OROS MPH 18 mg、36 mg改善行為舉止效果 (SKAMP-deportment) 改善率比較圖10
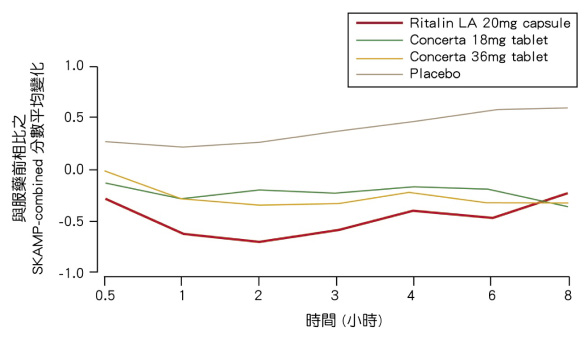
圖七 Ritalin LA 20 mg 與 OROS MPH 18 mg、36 mg 改善 ADHD 綜合症狀效果 (SKAMP-combine) 改善率比較圖10
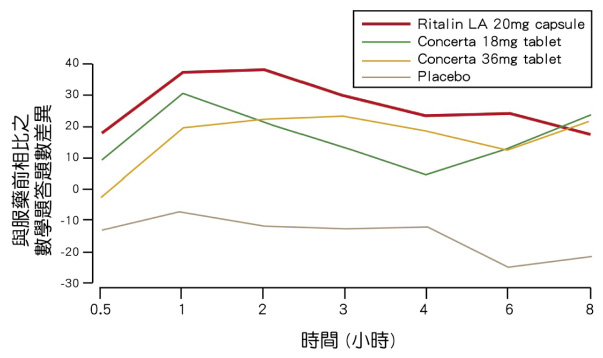
圖八 Ritalin LA 20 mg 與 OROS MPH 18 mg、36 mg 對數學問題答題數影響之比較圖10
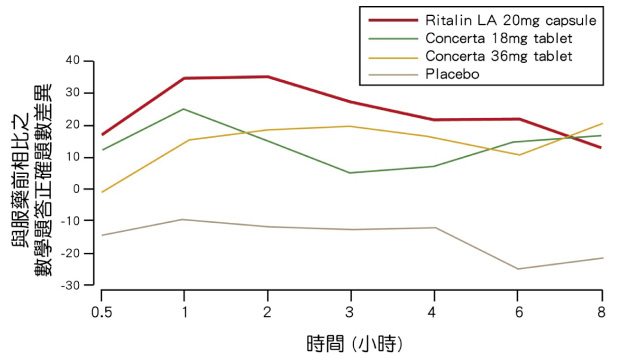
圖九 Ritalin LA 20 mg 與 OROS MPH 18 mg、36 mg 對數學問題答題正確數影響之比較圖10
三、 隨機、單盲、安慰劑對照、交叉實驗設計的臨床試驗11
一項隨機、單盲、安慰劑對照、交叉實驗設計的擬課堂臨床試驗比較 Ritalin LA 20 mg、40 mg 與 OROS MPH 18 mg、36 mg,對象為54名6至12歲依據 DSM-IV 診斷為 ADHD 的兒童。試驗的結果顯示,Ritalin LA 40 mg 在服藥0-4小時、0-8小時、0-12小時間,改善 ADHD 症狀之效果顯著優於 OROS MPH 36 mg 與安慰劑;服用 Ritalin LA 20 mg 後0-8小時之治療效果與 OROS MPH 18 mg、36 mg 相近,且具有良好耐受性。
伍、病人耐受性與安全性
一項評估 Ritalin LA 的療效及安全性的安慰劑對照、雙盲、平行設計的試驗中,試驗前四週單盲期的 Ritalin LA 劑量調整期間,發生率 > 5%的不良事件為頭痛、失眠、上腹部疼痛、食慾減退和厭食;在臨床試驗中為期兩週雙盲期間,Ritalin LA 治療組的受試者因治療而發生不良事件,且發生率 > 2%者為厭食與失眠。
陸、建議劑量與用量
一、劑量
Ritalin 的投藥量應根據病人臨床上的需要及反應而定。應由低劑量開始給與,每星期逐步增加。每日劑量不應超過40毫克。若本品與速效劑型合用時,所有不同劑型的 methylphenidate hydrochloride 總量不可超過每日60毫克。
二、建議用法
Ritalin LA 持續性藥效膠囊 (methylphenidate hydrochloride extended-release capsules) 每天一次,在早上投與,建議起始劑量為10毫克。劑量調整可依照所觀察到的耐受性及治療效果,每週增加10毫克,直至每日最大劑量40毫克。一天給與 Ritalin LA 持續性藥效膠囊一次,相較於總劑量相同的 Ritalin 錠劑,分二次給藥,二者的 methylphenidate 整體曝藥量 (AUC) 相當。
(一)一般建議用法
Ritalin LA 持續性藥效膠囊及膠囊內的藥粒不可磨碎、咀嚼或切割藥粒。
三、 轉換成 Ritalin LA 持續性藥效膠囊治療
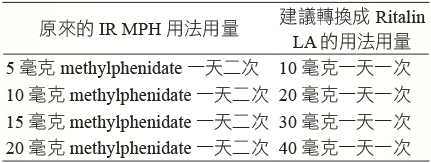
以 IR-MPH 治療換成 Ritalin LA 治療時的建議劑量如表二。
表二 IR-MPH 轉換為 Ritalin LA 之用法用量轉換表8,12
柒、結論
Methylphenidate 為治療孩童 ADHD 之主要用藥。在美國,為因應各種不同 ADHD 患者的需求,美國 FDA 陸續核准了 Ritalin SR、OROS MPH (Concerta)、Equasym XL 與 Ritalin LA 等多種 ER-MPH 製劑。這些 ER-MPH 各自都採用各種不同的緩釋技術,也各自呈現的各種不同的藥物動力學特性與療效;並沒有一個 ER-MPH 製劑的療效明顯地優於其它製劑,選擇 ER-MPH 製劑最重要的考量應該是以各種患者治療需求為出發點,為患者選擇最適合的製劑13。
Ritalin LA 是依據每日服用2次 IR-MPH 的藥物動力學特性設計的 ER-MPH,謝瓊慧與孟瑛如於2010年發表的研究顯示,每日服用1次 Ritalin 的學童佔全部服用 Ritalin 的58.3%,服用2次的佔31.8%,服用3次的佔9.8%;而服用 OROS MPH 的 ADHD 學童人數則佔了全部使用 MPH 成分的30.5%14。
Ritalin LA 讓國內的 ER-MPH 多了一個選擇,也讓醫師能在患者需要由 IR-MPH 轉換為 ER-MPH 時能依據患者治療的需求,給予患者最佳的醫療選擇。
SODAS Formulation Applied to the Analysis of Methylphenidate HCl
Chen-Ting Ku
Tsaotun Psychiatric Center Ministry of Health and Welfare
Abstract
Attention Deficit/Hyperactivity Disorder, ADHD) treatment can be divided into drug treatment, behavioral therapy and behavioral therapy medication merge three categories; NIH (National Institutes of Health, NIH) in ADHD treatment guidelines point out that the combined medication and behavioral therapy alone medication to control the symptoms of ADHD quite effective, and far superior to behavioral therapy; medication merge non-behavioral therapy to improve the core symptoms of ADHD, there are better results. There are domestic approved ADHD drugs methylphenidate (MPH) and atomoxetine are two of them belong to the psychostimulant methylphenidate on pharmacological classification (psychostimulants), is home to the main drug treatment of children with ADHD, because of its duration of action is only about four hours, can be divided into general formulations (IR-MPH) and long-acting formulation (ER-MPH) two kinds of forms on it.
Spheroidal Oral Drug Absorption System (SODAS) is a multi-particle developed by Elan Corporation, plc's multiparticulate technology, which includes the immediate release and sustained-release, fast-acting effect of the particles have a fast-acting, sustained release particles may be taking drugs after a certain time and then the drug release, the drug to reach and close to twice the blood drug concentration profile taken.
ER-MPH different sustained-release technology, show different dynamics and efficacy of the drug; and there is no effect of ER-MPH formulations significantly better than other agents, select ER-MPH formulations of the most important considerations should be based on a variety of patients demand as the starting point, select the most appropriate formulation for patients.
參考資料:
1.Diagnosis and Treatment of Attention Deficit Hyperactivity Disorder. NIH Consensus Statement 1998 Nov.
2. Pappadopulos et al: Medication adherence in the MTA: saliva methylphenidate samples versus parent report and mediating effect of concomitant behavioral treatment. J Am Acad Child Adolesc Psychiatry. 2009.48(5):501-10.
3. Thompson et al: Switching from immediate- to sustained-release psychostimulants in routine treatment of children with attention-deficit hyperactivity disorder. Psychiatric Bulletin. 2006. 30: 247-250.
4. Gormez et al: Switching from immediate release to sustained release methylphenidate in the treatment of children and adolescents with attention deficit/hyperactivity disorder. Eur Rev Med Pharmacol Sci. 2013. 17(17):2345-9.
5. Hosenbocus and Chahal.. A Review of Long-Acting Medications for ADHD in Canada. J Can Acad Child Adolesc Psychiatry. 2009.18(4):331-9.
6. B.Venkata Phani Deepthi.. Spheroidal Oral Drug Absorption System (SODOS). Journal of Global Pharma Technology. 2011,3(10):01-05.
7. Katherine A. Lyseng-Williamson, Gillian M. Keating.. Extended- Release Methylphenidate (Ritalin® LA). Drugs. 2002, 62(15):2251-9; discussion 2260-1.
8. Novartis Pharmaceuticals Corp. Ritalin LA (methylphenidate HCL) product monograph. East Hanover (NJ): Novartis Pharmaceuticals Corp. 2014.
9. Markowitz JS, Straughn AB, Patrick KS, et al: Pharmacokinetics of methylphenidate after oral administration of two modified-release formulations in healthy adults. Clin Pharmacokinet. 2003. 42 (4): 393-40.
10. Lopez et al: Comparative Efficacy of Two Once Daily Methylphenidate Formulations (Ritalin® LA™ and Concerta®) and Placebo in Children with Attention Deficit Hyperactivity Disorder Across the School Day. Pediatr Drugs. 2003.5 (8): 545-555.
11. Silva et al: Efficacy of Two Long-Acting Methylphenidate Formulations in Children with Attention-Deficit/Hyperactivity Disorder in a Laboratory Classroom Setting. J Child Adolesc Psychopharmacol. 2005. 15(4):637-54.
12. Markowitz, et al: Advances in the Pharmacotherapy of Attention-Deficit–Hyperactivity Disorder: Focus on Methylphenidate Formulations. Pharmacotherapy. 2003, 23(10):1281-1299.
13. Coghill et al: Long-acting methylphenidate formulations in the treatment of attention-deficit/hyperactivity disorder: a systematic review of head-to-head studies. BMC Psychiatry. 2013,13:237.
14. 謝瓊慧、孟瑛如。國小過動症學生之藥物治療調查研究。特教論壇。2010,12 (9期),047-062。

