摘要
不適當使用抗生素造成的問題不僅是醫療成本的增加,更可能使病人遭受不必要的不良反應與細菌抗藥性而增加治療的困難度。本研究藉由建立抗生素藥師與感染科醫師共同照護模式,依巡診方式評估廣效抗生素,以期瞭解區域教學醫院開立廣效抗生素的適當性。採取回溯性病例研究,分析院內在共照模式建立後,對廣效性抗生素處方執行藥事照護介入的情形,以 SPSS 24.0依照類別變相使用卡方檢定。
本研究共審查349位病人與626筆抗生素處方,以加護病房處方居多。經評估後,統計不適當抗生素處方的比例為42.8%,以處方 metronidazole 適當性明顯最低 (p = 0.000),其次依序為 carbapenems (p = 0.011) 與 penicillinase inhibitor combinations (p = 0.047);而 glycopeptides 雖不具有統計意義,但適當性趨勢也偏低 (p = 0.071)。醫療端對抗生素劑量調整的接受度為97.7%,而對更改藥物選擇的接受度僅有91.1%。比較研究前後藥師執行抗生素處方照護的介入行為,在與感染科醫師合作指導與討論下更能增進藥師在審查處方選擇的能力 (p = 0.000)。
期許醫院藥師能在共同照護模式下,提升抗生素藥事照護的品質,並進一步提高院內處方廣效性抗生素處方的合理性。
關鍵字: 抗生素、合理性、醫院藥師、clinical pharmacist、appropriate、antibiotic
壹、前言
抗生素管理常常面臨多種問題,如對病人死亡率或住院天數的影響等,雖然這些指標並無法直接反應抗生素管理的適當性,卻仍是造成醫院藥師執行抗生素介入時常面臨的挑戰1。本文描述一研究藉由臨床藥師與感染科醫師共同巡診評估抗生素,以瞭解區域教學醫院開立廣效抗生素的適當性,也將常見開方不當情形提供臨床審查參考,並分析抗生素藥師在執行處方照護上在此共同照護模式前後是否有不同。
貳、材料與方法
本文為回溯性病例研究,資料擷取自2015年8月至2016年8月間,抗生素藥師與感染科醫師共同評估抗生素處方的合適性。本研究前建立臨床藥師與感染科醫師共同照護模式,制訂評估抗生素審查規範後,執行住院病人抗生素處方的合理性評估,包括藥物劑量與藥物的選擇。每週定期與感染科醫師討論爭議的個案,並給予臨床醫師適當的回饋建議。
一、研究步驟
制訂審查規範與處方追蹤模式:針對非複雜性疾病,包括院內肺炎、腹腔內感染、血流感染與泌尿道感染等,建立標準劑量範圍並與感染科醫師達成劑量調整共識。藥師對抗生素處方的審查與評估,需依其感染症、共病症、培養結果以及肝、腎功能情形,逐筆登錄於 excel 中,並對建議處方追蹤臨床接受度與病情變化。
二、納入條件
開方廣效抗生素之成人住院者,並排除因嚴重疾病採取緩和療法的末期病人。廣效抗生素包括 penicillinase (PCNase) inhibitor combinations、3rd~4th cephalosporins、carbapenems、fluroquinolones、glycopeptides、metronidazole、fluconazole、tigecycline、colistin、daptomycin 與 linezolid。
三、結果指標
抗生素選擇與劑量的適當性。適當性的定義:(一)經驗性選擇的合適性;(二)經驗性給藥後依照培養證據作適當的調整;(三)合併藥品的必要性以及(四)劑量依照病人腎功能、肝功能與洗腎方式作適當改變;(五)感染症診治指引;(六)文獻報告。
四、統計方式
研究結果依照類別變相(一)不合理抗生素的類別與開方錯誤率;(二)研究前後與藥事照護介入類別的比率,利用電腦軟體 SPSS Statistics 24.0使用卡方檢定 (pearson chi square) 比較其差異,並且視p值低於0.05為顯著差異。
參、結果
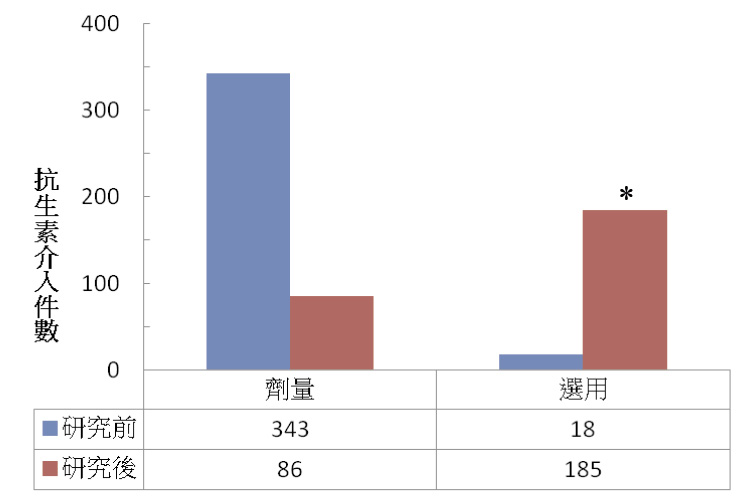
本研究主要審查單位為加護病房,共審查349位病人與626筆處方,其中加護病房處方筆數約占75%。統計不適當抗生素處方的比例為42.8%,加護病房高於一般病房 (表一),尤其對於藥物選用不當的問題甚是。醫療端對抗生素劑量調整的接受度為97.7%;然而,對更改藥物選擇的接受度為91.1%。相對於過去藥師大多數只介入抗生素劑量調整的情形,發現在研究後藥師介入抗生素選用的比率有顯著的增加 (圖一),研究前後分別為4.9%與68.2% p = 0.000),顯示透過團隊合作更能提升抗生素藥師把關合適處方的能力。抗生素藥師在處方劑量介入的比例雖然下降,但在有限的臨床服務量下也提高了經驗性劑量的合理性 (圖二),研究前後分別為23%與47.7%)。
表一 廣效性抗生素在不同病房的適當性
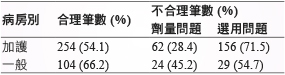
* Pearson 卡方檢定,p = 0.0000
圖一 研究前後藥師執行抗生素處方照護的介入行為
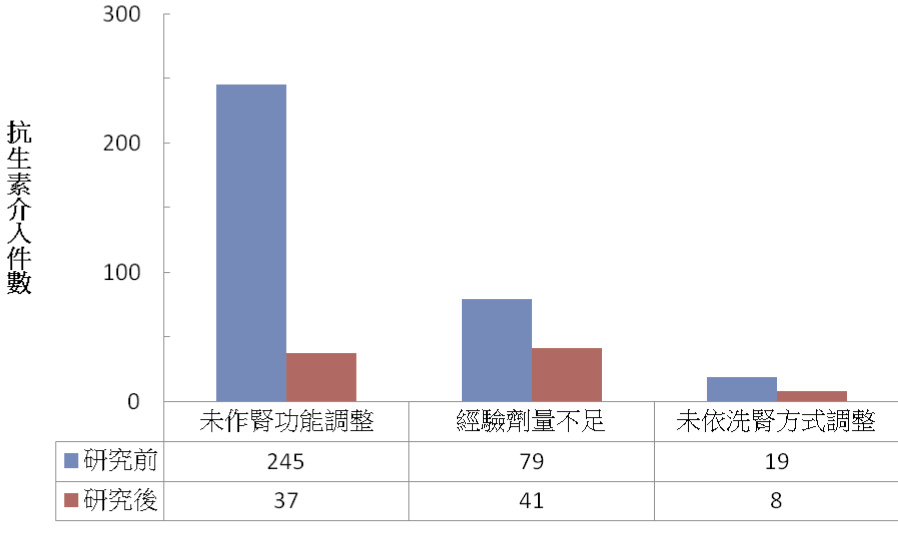
圖二 研究前後藥師介入抗生素劑量的原因
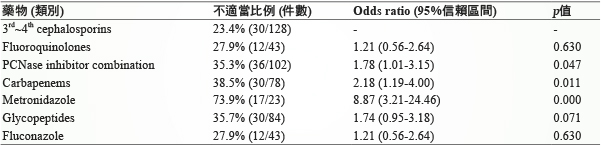
以 Odds ratio 統計分析抗生素開方類別與不適當的比例 (表二),處方 metronidazole 不適當性明顯最高 (p = 0.000),其次依序 為 carbapenems (p = 0.011) 與 PCNase inhibitor combinations (p = 0.047);而 glycopeptides 雖不具有統計意義,但不適當性趨勢也偏高 (p = 0.071)。
表二 Odds ratio 統計分析抗生素開方類別與不適當的比例
進一步分析各類抗生素「不必要使用」的問題主要如下:
一、PCNase inhibitor combinations
在排除厭氧菌與抗藥性細菌的情況下,應適當窄化抗菌範圍,以減少對腸道菌種的影響。
二、Carbapenems
應依照培養結果、宿主因素與臨床症狀降階至別類抗生素。適當的減少 carbapenems 使用,不僅可減少 CDAD (Clostridium difficile assiociated dissease) 發生率,更可降低相關抗藥性菌株的比例2。
三、Metronidazole
除了治療 Clostridium difficile assiociated disease (CDAD) 為合理使用 metronidazole 之外3,其他感染症若同時使用具有抗厭氧菌效果的抗生素時4,則需避免以減少不必要的雙重抗厭氧菌問題。具有抗厭氧菌效果的抗生素如 PCNase inhibitor combination (amoxicillin-clavulanate、ampicillin-sulbactam 與 piperacillin-tazobactam)、cephalosporins (cefoxitin、cefmetazone、flomoxef 與 cefoperazone-sulbactam)、carbapenems(ertapenem、imipenem-cilastatin、meropenem 與 doripenem)、moxifloxacin 與 tigecycline。
四、Glycopeptides
當判斷為血液檢體汙染而造成陽性血液培養報告時,不應持續使用 vancomycin 或 teicoplanin。當兩套血液培養只有一套或且為皮膚正常菌叢時,應懷疑為檢體污染而非感染5,停用 vancomycin 或 teicoplanin 以減少 vancomycin resistance enterococcus 的比例。
五、Fluconazole
當只有痰液培養或經由導尿管的尿液檢體有 Candida,若判斷為無症狀菌尿症時,不應持續使用 fluconazole。Candida 菌種常見於皮膚、呼吸道與腸胃道,尤其給予廣效性抗生素之後的培養可視為菌株篩選後 (collateral damage) 的結果,因此應謹慎使用 antifungal 藥品於上述情形6。
研究期間共有9人疑似為抗生素導致相關的不良反應:(一)心臟方面:一例心衰竭患者在使用 levofloxacin 期間發生 QT 延長;(二)血液方面:三例為使用 beta-lactams 造成血小板低下 (分別為 cefepime 2 例與 meropenem 1 例),且其中一例 (cefepime) 為長時間合併 vancomycin 造成全血球低下。另一例為使用 cefoperazone-sulbactam 造成凝血時間延長導致出血問題;(三)肝臟方面:一例使用 fluconazole 造成肝指數上升;(四)中樞方面:2例使用 carbapenems 影響 valproic acid 濃度而造成血中濃度不足 (分別為 ertapenem 與 meropenem),其中一例有癲癇發生;(五)腎功能方面:一例使用 vancomycin 期間造成腎功能惡化。上述不良反應症狀皆因停藥或改藥獲得緩解。
肆、討論
根據國外統計,抗生素開方不當約占20-50%7,而加護病房可能更高8。本研究在有限的收案審查下,顯示抗生素處方不適當是目前醫院感染管制需重視的問題。不適當處方包括藥物選擇失誤、劑量錯誤以及使用天數過長或不足,除了導致病人增加不良反應的機會之外9,更容易導致抗藥性菌種的發生。
經驗性抗生素選擇失誤是導致處方失當最主要的問題,加護病房開方人員更是在高度的工作負荷以及醫病關係壓力下,對工作環境的抗藥性細菌比例不瞭解,加上抗生素的開方限制太少等,無法處方正確的抗生素而導致開方錯誤10。
合理的抗生素使用需仰賴多方面考量,包括(一)對疾病作正確診斷;(二)依據培養盡可能窄化抗生素與(三)宿主因素;以及(四)非必要下不延長治療時間。同時,必須了解外科介入對深層感染症的治療更為重要11。體外試驗雖不一定反應真正治療的結果,配合臨床感染指標的監測下,對抗生素是否採合併療法、降階或窄化等,藥物敏感性試驗可提供相當的參考價值。另外,抗生素的劑量調整除了評估腎功能之外,也需留意(一)經驗性劑量的正確性與(二)各種透析方式對抗生素移除的比例,以防止感染治療失敗或避免增加不良反應。最後,依個別抗生素制定安全監測策略,可讓治療多一層安全的把關。
在現實的開方環境,為了減少專科訓練不足導致的不當處方,全職藥師可與感染科醫師共同合作,協助正確抗生素資訊的傳遞。並且,透過跨領域資訊的分享與溝通,讓藥師學習與臨床面對面討論,不僅可減少對處方不必要的猜測而增進審查效率,更可跳脫以往只對劑量思考的框架。面對抗藥性細菌與日俱增的威脅,期許醫院藥師能不負眾望,確實執行抗生素管理之職責。本研究計畫編號為 NTUHYL.105I005。
Investigation of Antimicrobial use in Regional Teaching Hospital
Shu-Chen Yang1, Pei-Ling Tsai1, Chin-Ju Chuang1, Lin-Chu Liao1, Chi-Ying Lin2
Department of Pharmacy1, Department of Infectious Disease2
National Taiwan University Hospital Yunlin Branch
Abstract
Inappropriate use of antibiotics may increase the risk of adverse effects and result in the emergence of resistant bacteria. For identifying the common problems in prescription of antibiotics in our hospital, we assess the rationale of hospitalized patients who received antibiotic therapy retrospectively. Clinical pharmacists collaborating with the infectious disease physician performed ward round every week that focused on patients who received broad-spectrum antibiotics from Augst 1,2015 to Augst 1,2016. Appropriateness of antibiotics use was recorded and assessed based on the clinical conditions of patients, results of image studies, evidences of microbiological studies, the prescriptions of antibiotics, including the spectrum of coverage, dosage, treatment duration and side effects. Pearson’s chi-square test is used to discover if there were a relationship between categorical variables (as percentages) by using the SPSS 24.0.
During the study period, 349 patients were treated with broad-spectrum antibiotics and total of 626 antibiotic prescriptions were evaluated. According to our assessment, 45.5% of antibiotics prescribed in our hospital were inappropriate. The most common error in antibiotic prescription was the combination use of metronidazole with broad-spectrum antibiotics that have anaerobic coverage, with rate as 8.87%(95% CI 3.21~24.46, p = 0.000).The rate of inappropriate use of carbapenems and penicillinase inhibitor combination were 2.18(95% CI 1.19~4.00, p = 0.0011) and 1.78(95% CI 1.01~3.15, p = 0.0047) respectively, higher than that of 3rd~4th cephalosporins.Our study also showed that there was a significant improvement of optimal antibiotic use regarding the dosage and choice of antibiotic after our intervention (p = 0.000).
Errors in antibiotic prescription including choice of drug, dosage and lack of de-escalation after microbiologic results available are common in hospital. Optimization of antibiotic use can be improved by setting up a collaboration team between clinical pharmacist and ID physician.
參考資料:
1.Akpan. M. R, Ahmad.R, Shebl. N. A, et al: A Review of Quality Measures for Assessing the Impact of Antimicrobial Stewardship Programs in Hospitals. Antibiotics (Basel) 2016; 5 (1).
2. Lew. K. Y., Ng.T. M., Tan. M, et al: Safety and clinical outcomes of carbapenem de-escalation as part of an antimicrobial stewardship programme in an ESBL-endemic setting. The Journal of antimicrobial chemotherapy 2015; 70 (4): 1219-25.
3. Nelson. R. L., Kelsey. P.,Leeman. H, et al: Antibiotic treatment for Clostridium difficile-associated diarrhea in adults. Cochrane Database Syst Rev 2011; (9), CD004610.
4. Wang. F. D., Liao. C. H., Lin. Y. T, et al: Trends in the susceptibility of commonly encountered clinically significant anaerobes and susceptibilities of blood isolates of anaerobes to 16 antimicrobial agents, including fidaxomicin and rifaximin, 2008-2012, northern Taiwan. Eur J Clin Microbiol Infect Dis 2014; 33 (11): 2041-52.
5. Weinstein. M. P.,Towns. M. L., Quartey. S. M, et al: The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis 1997; 24 (4): 584-602.
6. Pappas. P. G., Kauffman. C. A., Andes. D. R, et al: Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2016; 62 (4): e1-50.
7. Pollack. L. A., Srinivasan. A.: Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin Infect Dis 2014; 59 Suppl 3: S97-100.
8. Luyt. C. E., Brechot. N., Trouillet. J. L, et al: Antibiotic stewardship in the intensive care unit. Crit Care 2014; 18 (5): 480.
9. King. R. N., Lager. S. L.: Incidence of Clostridium difficile infections in patients receiving antimicrobial and acid-suppression therapy. Pharmacotherapy 2011; 31 (7): 642-8.
10. Calbo. E., Alvarez-Rocha. L., Gudiol. F, et al: A review of the factors influencing antimicrobial prescribing. Enferm Infecc Microbiol Clin 2013; 31 Suppl 4: 12-5.
11. Leekha. S., Terrell. C. L., Edson. R. S, et al: General principles of antimicrobial therapy. Mayo Clin Proc 2011; 86 (2): 156-67.
通訊作者:楊淑珍/通訊地址:雲林縣斗六市雲林路二段579號
服務單位:台大醫院雲林分院藥劑部藥師/聯絡電話:(O) 05-5323911 ext 5187

