摘要
臨床使用的藥物中,超過600個具有抗乙醯膽鹼 (anticholinergic) 活性。抗乙醯膽鹼藥物的作用機轉是拮抗週邊和中樞神經系統的毒蕈鹼 (muscarine) 接受器。約50%的老年人使用的藥物中至少有一個具有抗乙醯膽鹼作用。老年人對於抗乙醯膽鹼藥物較為敏感,易產生中樞副作用,例如:譫妄、認知和記憶障礙。研究顯示,老年人使用高活性抗乙醯膽鹼藥物的累積劑量越高,失智的發生風險越大。最常使用的高活性抗乙醯膽鹼藥物分類為三環抗憂鬱藥、第一代抗組織胺、作用於膀胱的抗乙醯膽鹼藥物。抗乙醯膽鹼藥物負載 (anticholinergic drug burden,ACh-B) 是指使用一種或多種具有抗乙醯膽鹼活性的藥物之累積總合。利用放射線同位素直接測量血中抗乙醯膽鹼活性是評估 ACh-B 最理想的作法,但是此方法昂貴且不切實際。目前,有多至10個衡量工具可用來評估 ACh-B。減少 ACh-B 最重要的策略是優先採用非藥物治療,盡量將藥物治療放在最後選項。已診斷為失智的病人應避免使用抗乙醯膽鹼藥物。藥師可建議醫師選擇沒有抗乙醯膽鹼活性或低活性之替代藥物來降低 ACh-B,俾使病人的用藥更加安全。
關鍵字: 抗乙醯膽鹼藥物、抗乙醯膽鹼藥物負載、anticholinergic drug burden
壹、前言
臨床使用的藥物中,超過600個具有抗乙醯膽鹼 (anticholinergic) 活性1。經由此作用可用來治療膀胱過動症、腸胃道痙攣、帕金森氏症;然而,第一代抗組織胺、三環抗憂鬱藥、某些抗精神病藥物,因其具有抗乙醯膽鹼副作用,造成病人服藥順從性不佳,反而會影響療效2。本文將針對抗乙醯膽鹼藥物做詳細探討。
貳、抗乙醯膽鹼藥物
抗乙醯膽鹼藥物的作用機轉是拮抗週邊和中樞神經系統的毒蕈鹼 (muscarine) 接受器。毒蕈鹼接受器有5個亞型:M1-M5,其中 M1和 M2接受器廣泛分布於腦中,若受到抑制會引起記憶和學習障礙;M3接受器在腦內的濃度低,若受到拮抗不會影響認知功能3。幾乎所有的抗乙醯膽鹼藥物對於毒蕈鹼接受器皆不具專一性,換言之,5個亞型都會阻斷3。抗乙醯膽鹼藥物引起中樞副作用之風險高低,取決於其穿過血腦屏障 (blood-brain barrier,BBB) 的能力以及與毒蕈鹼接受器結合的親和力3。舉例來說,amitriptyline 和 paroxetine 皆屬於高活性抗乙醯膽鹼藥物4,但是前者較易引起記憶障礙5。
參、抗乙醯膽鹼藥物的副作用
週邊副作用有口乾、眼睛乾澀、視力模糊、便秘、尿液滯留、心跳加快。中樞副作用有暈眩、鎮靜、意識混亂、譫妄、注意力不集中、認知障礙、失去記憶1,3,6。除此之外,老年人使用抗乙醯膽鹼藥物和跌倒以及死亡率增加有關1。
肆、老年人使用抗乙醯膽鹼藥物
約50%的老年人在其使用的藥物中至少有一個具有抗乙醯膽鹼作用3。由於老化會改變藥物動力學和藥效學、增加 BBB 的通透性、降低腦內經由乙醯膽鹼媒介的傳遞,因此老年人對於抗乙醯膽鹼藥物較為敏感,較易產生中樞副作用,例如:譫妄、認知和記憶障礙2。
伍、抗乙醯膽鹼藥物與失智
抗乙醯膽鹼藥物的中樞副作用可能會被誤判為失智或輕度認知障礙。研究發現,被懷疑是失智的病人,估計其中2-12%的患者並不是真正的失智,而是因為使用抗乙醯膽鹼藥物所致6。一前瞻性世代研究長期使用抗乙醯膽鹼藥物與失智的關聯性,共收錄3434位65歲以上老人,檢視他們過去10年的用藥,計算其使用高活性抗乙醯膽鹼藥物的累積劑量,平均追蹤7.3年,結果顯示累積劑量越高,失智的發生風險越大2。最常使用的高活性抗乙醯膽鹼藥物分類為三環抗憂鬱藥、第一代抗組織胺、作用於膀胱的抗乙醯膽鹼藥物2。
陸、評估抗乙醯膽鹼藥物負載
抗乙醯膽鹼藥物負載 (anticholinergic drug burden,以下簡稱 ACh-B) 是指使用一種或多種具有抗乙醯膽鹼活性的藥物之累積總合7。利用放射線同位素直接測量血中抗乙醯膽鹼活性是評估 ACh-B 最理想的作法,但是此方法昂貴且不切實際7。目前,有多至10個衡量工具可用來評估 ACh-B7。這些衡量工具孰優孰劣並無共識。研究發現,常用的5個衡量工具:Anticholinergic Cognitive Burden (ACB) Scale、Anticholinergic Drug Scale (ADS)、Anticholinergic Risk Scale (ARS)、Drug Burden Index anticholinergic component (DBI-ACh)、Summated Anticholinergic Medications Scale (SAMS),彼此一致性並不高8。Durán 等人依據7個有積分的衡量工具,定出47個高活性抗乙醯膽鹼藥物 (表一)1,和 Beers Criteria 列出的高活性抗乙醯膽鹼藥物相比 (表二)4,兩者仍有相當的差異性 (表一的47個藥物中有11個未出現在表二,而表二的52個藥物中有16個未出現在表一)。值得一提的是常用來治療帕金森氏症的藥物 bipediden,雖具有高度的抗乙醯膽鹼活性,但是卻未列入7。
表一 高活性抗乙醯膽鹼藥物1

表二 Beers Criteria 列出的高活性抗乙醯膽鹼藥物4

柒、減少抗乙醯膽鹼藥物負載
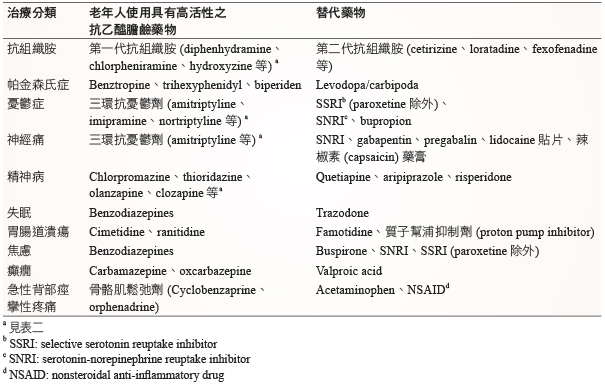
如何減少 ACh-B?最重要的策略是優先採用非藥物治療,盡量將藥物治療放在最後選項。例如:治療失眠可先建立良好的睡眠衛生 (sleep hygiene)、憂鬱症採取認知行為治療、疼痛選擇針灸或復健治療、行為異常者使用音樂治療9。已診斷為失智的病人應避免使用抗乙醯膽鹼藥物,特別是阿茲海默症 (Alzheimer's disease) 患者正在服用乙醯膽鹼酯酶抑制劑 (acetylcholinesterase inhibitor,AChEI) 時,因為抗乙醯膽鹼藥物會拮抗 AChEI 的藥理作用6。應盡量減少 ACh-B,尤其是老年人的用藥。表三列出可減少 ACh-B 之建議替代藥6,9。使用抗精神病藥物或三環抗憂鬱劑的患者,當轉換成其他替代藥時,注意原本使用的藥物需要一個月的時間降低劑量停藥10。
表三 可減少抗乙醯膽鹼藥物負載的建議替代藥6,9
捌、結論
具有抗乙醯膽鹼作用的藥物在臨床上的使用相當普遍,但是它們有潛在的風險,特別是用在老年族群。當老年人同時使用多種藥物時,其中可能會含有一個或多個抗乙醯膽鹼藥物,導致累積之 ACh-B。老年人對於 ACh-B 較為敏感,易產生中樞副作用,引發譫妄、認知和記憶障礙。研究也發現 ACh-B 越高,失智的發生風險越大。因此,身為醫療團隊成員之一的藥師有責任去審視處方,盡量減少 ACh-B,可建議醫師選用沒有抗乙醯膽鹼活性或低活性的替代藥物,俾使病人的用藥更加安全。
Anticholinergic Drug Burden
Chi-Yuan Cheng, Tzu-Cheng Tsai
Department of Pharmacy, Chang Gung Memorial Hospital, Linkou
Abstract
More than 600 drugs in clinical recognized to have anticholinergic activity. Anticholinergic drugs act on the muscarinic receptors in the peripheral and central nervous systems. About 50% of the elderly population uses at least one medication with anticholinergic effect. Older adults may be more sensitive to anticholinergic effects in the central nervous system and produce central adverse events such as delirium, cognitive and memory impairment. A study had shown that higher cumulative doses of drugs with strong anticholinergic properties use in the elderly was associated with an increased risk for dementia, and the most common anticholinergic classes used were tricyclic antidepressants, first-generation antihistamines, and anticholinergic drugs acting on the bladder. Anticholinergic drug burden (ACh-B) refers to the cumulative effect of taking one or more drugs with anticholinergic activity. Direct measurement of serum anticholinergic activity by radioisotopes assay is the best way in determining a patient’s ACh-B; however, it is expensive and impractical. At present, up to 10 scales are applying to estimate ACh-B. To reduce ACh-B, non-pharmacologic options are prior to drug treatment. Patients who diagnosed with dementia should not use anticholinergic drugs. Pharmacists may advise physicians to choose alternative medications with no or low-risk anticholinergic activity to minimize ACh-B to improve patient safety.
參考資料:
1.Durán CE, Azermai M, Vander Stichele RH: Systematic review of anticholinergic risk scales in older adults. Eur J Clin Pharmacol 2013;69:1485-96.
2. Gray SL, Anderson ML, Dublin S, et al: Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med 2015;175:401-7.
3. Kersten H, Wyller TB: Anticholinergic drug burden in older people's brain-how well is it measured? Basic Clin Pharmacol Toxicol 2014;114:151-9.
4. Fick DM, Semla TP, Beizer J, et al: American Geriatrics Society 2015 updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2015;63:2227-46.
5. Chew ML, Mulsant BH, Pollock BG, et al: Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc 2008;56:1333-41.
6. López-Álvarez J, Zea Sevilla MA, Agüera Ortiz L, et al: Effect of anticholinergic drugs on cognitive impairment in the elderly. Rev Psiquiatr Salud Ment 2015;8:35-43.
7. Villalba-Moreno AM, Alfaro-Lara ER, Santos-Ramos B: Anticholinergic risk: Use and limitations of anticholinergic scales. Eur J Intern Med 2015;26:e65-6.
8. Naples JG, Marcum ZA, Perera S, et al: Concordance between anticholinergic burden scales. J Am Geriatr Soc 2015;63:2120-4.
9. Hanlon JT, Semla TP, Schmader KE: Alternative medications for medications in the use of high-risk medications in the elderly and potentially harmful drug-disease interactions in the elderly quality measures. J Am Geriatr Soc 2015;63:e8-e18.
10. O'Donnell LK, Gnjidic D, Nahas R, et al: Anticholinergic burden: considerations for older adults. Journal of Pharmacy Practice and Research 2017;47:67-77.
通訊作者:鄭吉元/通訊地址:桃園市龜山區復興街5號
服務單位:林口長庚紀念醫院藥劑部藥師/聯絡電話:(O) 03-3281200 ext 2915

