摘要
氫離子幫浦抑制劑 (proton pump inhibitors,PPIs) 已經成為胃食道逆流 (gastroesophageal reflux disease,GERD) 和消化性潰瘍 (peptic ulcer disease) 的主流藥品。在過去幾十年中,許多文獻都提出有關使用 PPIs 嚴重不良事件的問題,包括腎毒性的疑慮。但證據資料不足以建立 PPIs 和這些事件之間的因果關係。多數的病人使用 PPIs 的整體治療效益和生活質量的改善明顯大於潛在的危害,但開立處方時沒有明確臨床適應症,可能會增加病人 PPIs 使用的風險。
關鍵字: 氫離子幫浦抑制劑、腎毒性、PPIs、Nephrotoxicity
壹、前言
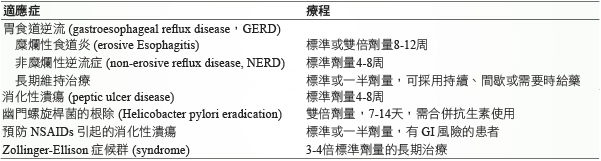
Omeprazole 是第一個氫離子幫浦抑制劑 (proton pump inhibitors,PPIs) 在1989年上市,其他的 PPIs (lansoprazole、rabeprazole、pantoprazole、esomeprazole 及 dexlansoprazole) 也陸續問世1,相較於 Histamine-2接受器拮抗劑 (histamine2-receptor antagonists,H2RAs)、合成前列腺素類似物 (synthetic prostaglandin analogs) 及抗膽鹼藥 (anticholinergics),PPIs 有良好的耐受性、卓越的安全性以及更佳的胃酸分泌抑制效果2,很快地成為 GERD 和消化性潰瘍的主流藥品 (表一)1-3,2009年的美國門診醫療調查中 PPIs 的處方張數從1995年的小於5張處方 (以每千人的 GERD 相關診次計算) 到2006年的43.9張,足足超過八倍的增加,因而 PPIs 的使用變得非常普遍,PPIs 的處方開始延長使用週期,有些甚至變成終身使用,這也潛在地衍生出 PPIs 在長期使用的安全性問題4。
表一 PPIs 常見的適應症1-3
貳、PPIs 的長期安全性
PPIs 的常見副作用是腹痛、便秘、腹瀉、腹脹、噁心、頭痛、眩暈、皮疹,發生率約1-3%,在個別 PPIs 之間並無明顯差異3。美國健康與營養體檢調查 (National Health and Nutrition Examination Survey,NHANES) 中,PPIs 的使用率從1999年的3.9%到2012年7.8%,同一時期,PPIs 相關不良反應的報告數量也是增加一倍5,主要是病例對照研究 (case control studies) 和統合分析 (meta-analysis);美國 FDA 也發布一些 PPIs 使用上的警訊,包括長骨骨折 (long bone fractures)、與氯吡格雷 (clopidogrel) 交互作用、腸道感染 (enteric infections) 和低鎂血症 (hypomagnesaemia)…等。最近,心血管事件、腎臟疾病和失智症 (dementia) 相關的問題也再度被提出6;另外即使有較便宜的學名藥配方,藥品的支出成本增加仍是一個問題3。
參、PPIs 引起的急性腎臟損傷
Omeprazole 在1992年就有相關急性間質性腎炎 (acute interstitial nephritis,AIN) 的觀察發表,後續其他的 PPIs 也有相關的案例報告7;和其他藥品一樣,可能是藥品本身和/或代謝物沉積在腎小管間質形成半抗原 (hapten) 或直接刺激T細胞造成免疫反應而誘發 AIN7;但 PPIs 誘發 AIN 在臨床上容易忽略,通常未警覺到 PPIs 會誘發 AIN4,再者其臨床表徵少有典型過敏反應 (< 10%)4,7:大約少於一半的病人會發燒、少於10%有皮疹表現、大約1/3有嗜酸性白血球過多 (eosinophilia),多半是非特異性主訴,例如疲勞 (fatigue)、噁心 (nausea) 和虛弱 (weakness)7,以及發生時間的變異性比較大,從服藥後的1星期到18個月都有可能,平均10-13星期4,7,8,這和其他藥品的發生時間10-14天不一樣7。
常見誘發 AIN 的三種藥品分別是 antibiotics、PPIs 及 NSAIDs8,9;特別要注意的是 PPIs 相較於 antibiotics 及 NSAIDs 病人的年齡較大 (71 vs 61 vs 52歲)、藥品曝露時間較久 (161 vs 13 vs 99天)、開始使用類固醇治療 (34 vs 8 vs 12.5天) 及腎臟切片 (33 vs 7 vs 11天) 的時間點也都相對地較慢9。所以臨床醫生及藥師應了解使用 PPIs 有發生 AIN 的風險,使用時應監測並減少不適當地使用 PPIs,AIN 發生時應盡快停用懷疑藥品9。
肆、PPIs 引起的慢性腎臟損傷
除了 AIN 之外,這幾年也陸續有些 PPIs 導致慢性腎臟疾病 (chronic kidney disease,CKD) 的研究發表,10,482人的動脈粥樣硬化風險社區研究 (atherosclerosis risk in communities study,ARIC study),收納腎小球濾過率 (glomerular filtration rate,eGFR) 大於等於60 mL/min 的受試者,初次訪視在1996年2月至1999年1月,追踪受試者至2011年12月,使用 PPIs 的受試者是較肥胖及較多併用降血壓藥、利尿劑、aspirin 及 statins,使用 PPIs 比未使用者發生 CKD 的風險增加45%,風險比值 (hazard ratio,HR) 是1.45(1.11-1.90, P = 0.006),其複製試驗 Geisinger 健康系統模擬世代 (Geisinger health system replication cohort,GHSR cohort) 收納248,751人,也是使用 PPIs 增加發生 CKD 的風險,HR 是1.2(1.15-1.26, P < 0.001);當根據人口統計學,社會經濟學和臨床變量進行調整時,使用 PPIs 的風險亦是較高,分別為 HR 1.50(1.14-1.96, P= 0.003) 和1.17(1.12-1.23, P < 0.001),PPIs 使用與 CKD 發生的關聯性仍然存在;兩個試驗都以 H2RAs 進行陰性對照 (negative control),HR 分別是1.15(0.98-1.36, P = 0.10) 及0.93(0.88-0.99, P =0.03) 和作為活性比較藥 (active comparator),HR 分別是1.39(1.01-1.91, P = 0.05) 及1.29(1.19-1.40, P < 0.001),H2RAs 並未顯示增加 CKD 的發生風險;在 GHSR cohort,一天服用兩次 PPIs 的 HR 是1.46(1.28-1.67, P < 0.001) 有較高 CKD 風險,相對於一天服用一次的 HR 1.15(1.09-1.21, P < 0.001),所以 PPIs 增加 CKD 風險和劑量相關10。另外,兩個試驗也評估 PPIs 與急性腎臟損傷 (acute kidney injury,AKI) 的相關性,結果分別是使用 PPIs 比未使用者增加 AKI 發生的風險72%(HR=1.72;1.28-2.30, P < 0.001) 和30%(HR =1.30;1.21-1.40, P < 0.001);HR 經過調整後的比值是1.64(1.22-2.21, P < 0.001)、1.31(1.22-1.42, P < 0.001),這顯示使用 PPIs 對於 CKD 或 AKI 的發生都是獨立的風險因素10。
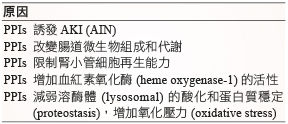
PPIs 造成 CKD 一般認為可能和發生過 AIN 有關,約30-70%病人 AIN 之後腎功能並沒有完全恢復,可能是急性發炎後快速進展成纖維化,尤其在診斷或治療延誤的狀況11。而使用 PPIs 導致 CKD 之前是否一定發生過 AIN?又或者有其他原因造成 CKD?一個採用美國退伍軍人資料庫 (the US department of veterans affairs databases) 所做的研究,收納 eGFR 大於60 mL/min 的受試者,追蹤5年,比較使用 PPIs 和 H2RAs 的長期腎臟結果 (long-term kidney outcomes),PPIs 使用增加 eGFR < 60 mL/min/1.73 m2,HR 1.19(1.15-1.24)、發生 CKD,HR 1.26(1.20-1.33)、eGFR 下降 > 30%,HR 1.22(1.16-1.28)、發生末期腎臟病 (end stage renal disease,ESRD) 或 eGFR 下降 > 50%,HR 1.30(1.15-1.48) 等慢性腎臟事件 (chronic renal event) 的風險;另外利用在試驗的不同時間點來排除曾經發生過 AKI 的受試者,結果也是增加慢性腎臟事件的風險,中介分析 (mediation analysis) 的結果呈現 AKI 造成慢性腎臟事件的風險大約占44-46%,也就是約一半的慢性腎臟事件可能由其他原因造成的 (表二)12,臨床上若只用 AKI 來監測慢性腎臟事件的發生是不足夠的;在評估 PPIs 暴露累積時間和慢性腎臟事件的分析中也發現有分級關聯性,當 PPIs 曝露時間越長 (≦ 30-720天) 發生慢性腎臟事件的風險隨之升高,所以 PPIs 的使用週期也應當注意,避免不必要的使用12。
表二 PPIs 造成慢性腎臟事件的原因12
伍、PPIs 的使用評估及建議
不論是腎臟毒性或是其他的毒性,像是失智症 (dementia)、骨折 (bone fracture)、心肌梗塞 (myocardial infarction)、小腸細菌過度增生 (small intestinal bacterial overgrowth)、自發性腹膜炎 (spontaneous bacterial peritonitis)、困難梭狀芽孢桿菌感染 (clostridium difficile infection)、肺炎 (pneumonia)、微量營養素缺乏 (micronutrient deficiencies)、胃腸道惡性腫瘤 (gastrointestinal malignancies) 等1,5,雖然研究結果顯示與 PPIs 的使用有關,不過受限於多為觀察性研究,沒有足夠的證據力來確定因果關係,所以臨床上並不會大幅度的修正使用方式1,3,6;然而這些問題主要源自於 PPIs 長期的過度使用,經常從住院開始使用,出院後繼續處方 PPIs,可能已經不具有使用的適應症,其中最多是低風險病人預防上腸胃道出血的使用3;另外由於共病 (multiple comorbidities) 和併用藥品較多,所以這個問題在老年人可能更危險3。住院病人不適當的 PPIs 處方比例:美國65%、澳洲63%、紐西蘭40%、義大利68%、愛爾蘭33%;馬來西亞的針對預防性胃酸抑制療法(acid suppression therapy,AST) 也有58.1%無適應症13,為了讓 PPIs 療效與安全獲得最佳的平衡,應當適時監控 PPIs 的處方行為,才能兼顧療效與風險1,2,3,5,14:
一、不要在沒有適應症的狀況下使用PPIs,讓用藥安全有保障。
二、多數適應症是有治療期限的 (表一)1-3,完成療程時,就應該停用 PPIs;當無法停用 PPIs,應該重新鑑別診斷,並且週期性地評估病人的整體狀況,確認是否還有用藥的需求,可以考慮嘗試不同的劑量策略3,5,14,以達到停用 PPIs 的目標:(一)持續 (continuous):PPIs 繼續使用,劑量不變、(二)減量 (decrease to lower dose):PPIs 繼續使用,但減少劑量、(三)需要時 (on-demand,as needed):療程結束時 PPIs 停用,症狀發生時再重新用藥、(四)換成 H2RAs 取代 PPIs。
其中依目前指引的推薦等級,減量及需要時使用是強烈推薦的方式;相較而言,以H2RAs 取代 PPIs 的推薦等級比較薄弱14。
三、必須長期使用 PPIs 的狀況 (表一)1-3,應該使用最小的有效劑量,可以減少潛在的安全性問題,同樣的也可以嘗試不同的劑量策略,期望能夠達到停用 PPIs,治療期間也是要週期性地評估病人的整體狀況3,5,14。
四、由於目前缺乏證據支持,以下狀況是不需要使用 PPIs3:(一)單獨使用類固醇或抗凝血劑時,使用 PPIs 為了提供胃保護 (gastroprotection) 作用、(二)預防肝硬化的高壓性胃病 (hypertensive gastropathy) 發生出血、(三)急性胰臟炎時,PPIs 的使用對於病程 (例如:縮短住院時間、開始進食或疼痛緩解的時間) 並無明顯改善。
五、慢性胰臟炎患者則建議有脂肪痢 (steatorrhea) 或對酶替代療法 (enzyme replacement therapy) 無反應者可使用標準劑量的 PPIs3。
六、一般情況下,老年人使用 PPIs 避免超過8周15。
七、在沒有適當證據的基礎下,使用 PPIs 不建議常規補充益生菌 (probiotics) 預防感染;鈣、B12、鎂的補充依照每日建議量 (recommended dietary allowance,RDA) 即可;骨密度、腎功能、鎂、B12…等檢測也照一般臨床需求即可5。
陸、結論
PPIs 是治療胃酸相關疾病不可替代的藥品,然而沒有一個藥品是絕對安全的,雖然目前的證據資料不足以建立 PPIs 和這些不良事件之間的因果關係,但換個角度來看,它也是一個 PPIs 使用的警訊,提醒我們 PPIs 使用上要更謹慎,多數的病人使用 PPIs 整體治療效益和生活質量的改善明顯大於潛在的危害;但是沒有明確臨床適應症或是長期使用,只會增加 PPIs 處方的風險。
Nephrotoxicity of Proton Pump Inhibitors
Chia-Hui Lin1, Chih-Kuei Lu2
Department of Pharmacy, Chang Gung Memorial Hospital, Linkou1
Department of Pharmaceutical Materials Management,
Chang Gung Memorial Hospital, Taoyuan2
Abstract
PPIs represent the mainstay of medical treatment of esophageal manifestations of GERD and peptic ulcer disease. In the past decades, numerous reports have raised questions about major adverse events related to the use of PPIs, including nephrotoxicity. There is insufficiency of evidence to establish causal relationships between PPI therapy and those events. The overall benefits of treatment and improvement of quality of life significantly outweigh potential harms in most patients. However, the prescription of PPIs without any clear indication may increase the risk of their adverse events.
參考資料:
1.Vaezi MF, Yang YX, Howden CW: Complications of Proton Pump Inhibitor Therapy. Gastroenterology 2017;153:35-48.
2. Strand DS, Kim D, Peura DA: 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017;11(1):27-37.
3. Scarpignato C, Gatta L, Zullo A: Effective and safe proton pump inhibitor therapy in acid-related diseases – A position paper addressing benefits and potential harms of acid suppression. BMC Med 2016;14:179-213.
4. Arora P, Gupta A , Golzy M, et al: Proton pump inhibitors are associated with increased risk of development of chronic kidney disease. BMC Nephrol 2016;17:112-9
5. Freedberg DE, Kim LS, Yang YX: The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology 2017;152:706-15.
6. Schnoll-Sussman F, Katz PO: Clinical Implications of Emerging Data on the Safety of Proton Pump Inhibitors. Curr Treat Options Gastro 2017;15:1-9.
7. Moledina DG, Perazella MA: PPIs and kidney disease: from AIN to CKD. J Nephrol 2016;29 (5):611-6.
8. Nast CC: Medication-Induced Interstitial Nephritis in the 21st Century. Adv Chronic Kidney Dis. 2017;24(2):72-9.
9. Muriithi AK, Leung N, Valeri AM, et al: Biopsy-Proven Acute Interstitial Nephritis, 1993-2011: A Case Series. Am J Kidney Dis. 2014;64(4):558-66.
10. Lazarus B, Chen Y, Wilson FP, et al: Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease. JAMA Intern Med. 2016;176(2):238-46.
11. Xie Y, Bowe B, Li T, et al: Proton Pump Inhibitors and Risk of Incident CKD and Progression to ESRD. J Am Soc Nephrol 2016;27:3153-63.
12. Xie Y, Bowe B, Li T, et al: Long-term kidney outcomes among users of proton pump inhibitors without intervening acute kidney injury. Kidney Int 2017; 91(6):1482-94.
13. Ai L. OH, Andrew GT, Hui SP, et al: Indication of acid suppression therapy and predictors for the prophylactic use of proton pump inhibitors vs. histamine-2 receptor antagonists in a Malaysian tertiary hospital. Pharm. Pract. 2015;13(3):633-8.
14. Farrell, B, Pottie K, Thompson W, et al: Deprescribing proton pump inhibitors Evidence-based clinical practice guideline. Can Fam Physician 2017;63:354-64.
15. By the American Geriatrics Society 2015 Beers Criteria Update Expert P.: American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 2015;63:2227-46.
通訊作者:林佳慧/通訊地址:桃園市龜山區復興街5號
服務單位:林口長庚醫院藥劑部藥師/聯絡電話:(O) 03-3281200 ext 3539

