第二型糖尿病的特徵是高血糖、胰島素阻抗、胰島素分泌異常,治療的目標是預防或延緩併發症並維持生活品質。美國糖尿病與歐洲糖尿病協會於2018年更新了關於第二型糖尿病管理的聲明,建議在慢性腎臟疾病、心臟衰竭、動脈粥狀硬化的心血管疾病病人使用 SGLT-2i (Sodium-glucose co-transporter-2 inhibitor) 是有益的。評估 SGLT-2i 對心血管影響的隨機雙盲臨床試驗:在併有心血管疾病或心血管疾病風險的第二型糖尿病患者,使用 empagliflozin 及 canagliflozin 與安慰劑相比顯示降低主要不良心血管事件,而 dapagliflozin 顯示則無差異。文內同時分析觀察性研究結果。再者糖尿病是引起慢性腎臟疾病的風險因子,本主題將論述 SGLT-2抑制劑使用於第二型糖尿病對心血管及腎臟的影響。
關鍵字:SGLT-2抑制劑、心血管、腎臟
壹、前言
目前第二型糖尿病的治療方法主要為增加胰島素可用性、增加胰島素的敏感性、延遲胃腸道碳水化合物的運送和吸收、增加尿糖排泄1。自從 rosiglitazone 引發心血管風險的爭議後,美國食品衛生管理局 (US Food Drug Administration;USFDA) 於2008年起要求之後所有新的糖尿病藥品須以高風險的第二型糖尿病人進行「主要不良心血管事件」(major adverse cardiovascular events;MACE) 為試驗終點的研究。MACE 包含心血管死亡 (cardiovascular death),心肌梗塞 (myocardial infarction;MI),以及缺血性腦中風 (ischemic stroke)。研究設計必須是不輸給安慰劑的非劣性研究 (non-inferiority trial),定義為風險 (hazard ratio;HR) 小於1.3倍,且達95%信賴區間作為標準2。
2018年10月美國糖尿病學會 (American Diabetes Association;ADA) 與歐洲糖尿病學會 (European Association for the Study of Diabetes;EASD) 依據最新的臨床研究結果,發表共同聲明。建構以病人為中心的治療計畫,衛教病人自我管理與參與治療決策的討論。運用共享決策的模式 (Shared decision making;SDM),共同擬定治療計畫,確實執行並定時評估成效,調整與更新執行的細項,包括生活習慣的改變及藥物治療的選擇。治療藥物 metformin 維持一線選擇,而二線用藥的選擇,先考量病人是否有動脈硬化的心血管疾病、心臟衰竭、慢性腎臟疾病,這群病人因死亡率與相關風險因子增加,治療上須更積極的介入。腎功能正常,可使用 SGLT-2i (Sodium-glucose co-transporter-2 inhibitor),若腎功能不佳,考慮使用 GLP-1(glucagon-like peptide-1) 類似物3。
2018年11月 Wiviott 等人發表了 dapagliflozin 使用於第二型糖尿病人的心血管影響。目前臨床上主要使用的三個 SGLT-2i 皆有大型的上市後研究探討用於併有心血管疾病 (cardiovascular disease;CVD) 的高風險病人的影響。除了隨機雙盲試驗外,運用大型醫療資料庫的觀察性研究以更完整的評估 SGLT-2i 的心血管安全性。
另一個與糖尿病互為風險因子的疾病--慢性腎臟病,上市後研究亦有探討相關議題。本文將論述 SGLT-2i (dapagliflozin, empagliflozin, canagliflozin) 使用於第二型糖尿病對心血管及腎臟的影響。
貳、SGLT-2i 對心血管的影響
探討 SGLT-2i 使用於第二型糖尿病對心血管影響的大型臨床試驗皆為多中心、隨機雙盲、安慰劑對照試驗。分別為 DECLARE (Dapagliflozin Effect on Cardiovascular Events)4、EMPA-REG (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients-Removing Excess Glucose)5、CANVAS (Canagliflozin Cardiovascular Assessment Study)6。三個研究收納的病人基本資料比較 (表一),收案族群中皆包含亞洲4-6。三個研究在 CVD 的病人收納比例略有不同:EMPA-REG 幾乎都是過去已有冠狀動脈疾病或中風史;CANVAS 及 DECLARE 各納入約六成及四成的有 CVD 的病人,其餘為有兩個以上心血管疾病風險因子者。
表一 SGLT-2i 對心血管影響試驗的病人基本資料比較表4-6
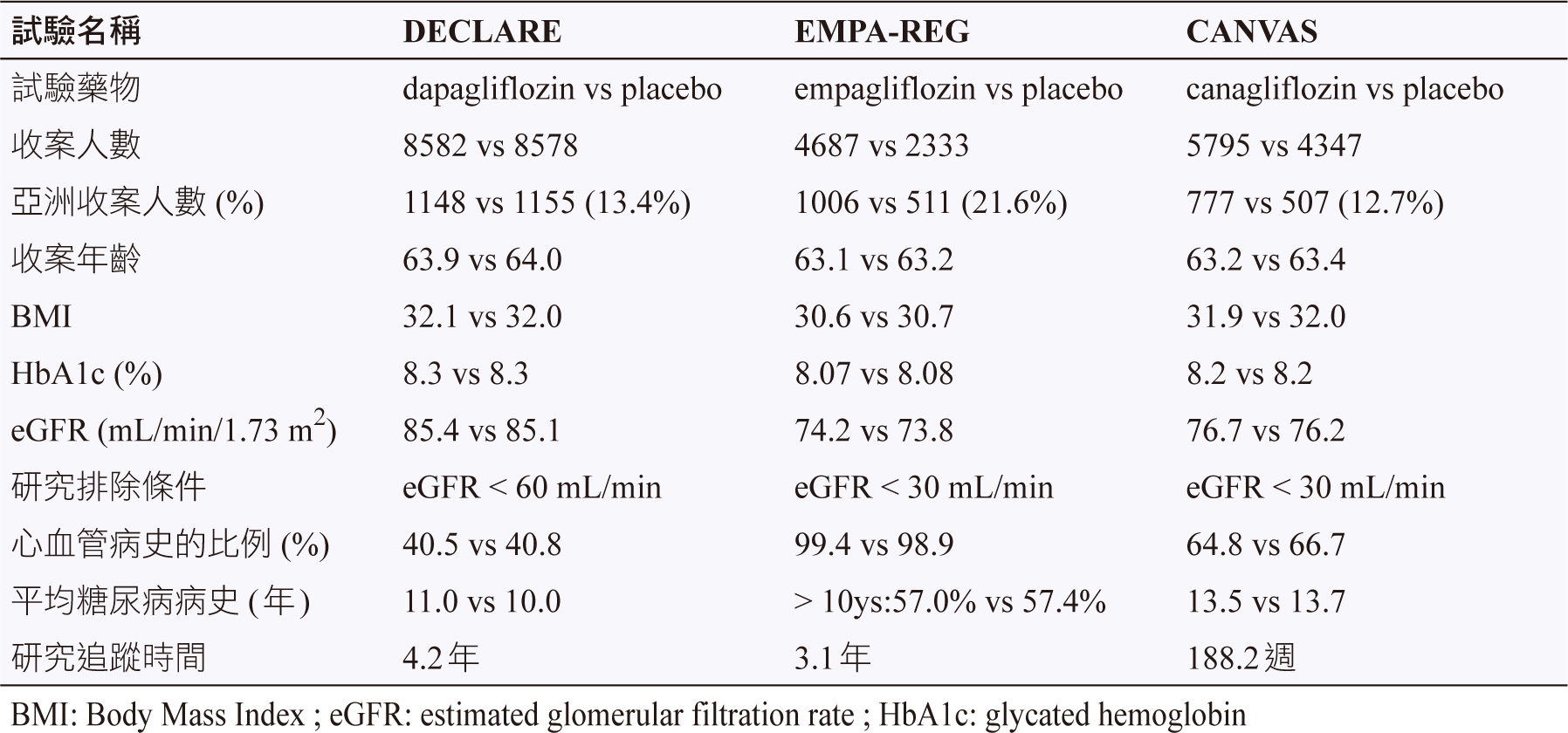
另一個差異為研究對象的排除條件,因為腎功能的限制,DECLARE 排除 eGFR < 60 mL/min,而另兩者排除 eGFR < 30 mL/min 的病人4-6。然而在台灣,目前 empagliflozin 和 canagliflozin 建議在 eGFR > 45 mL/min 以上使用,dapagliflozin 建議在 eGFR > 60 mL/min 以上使用。
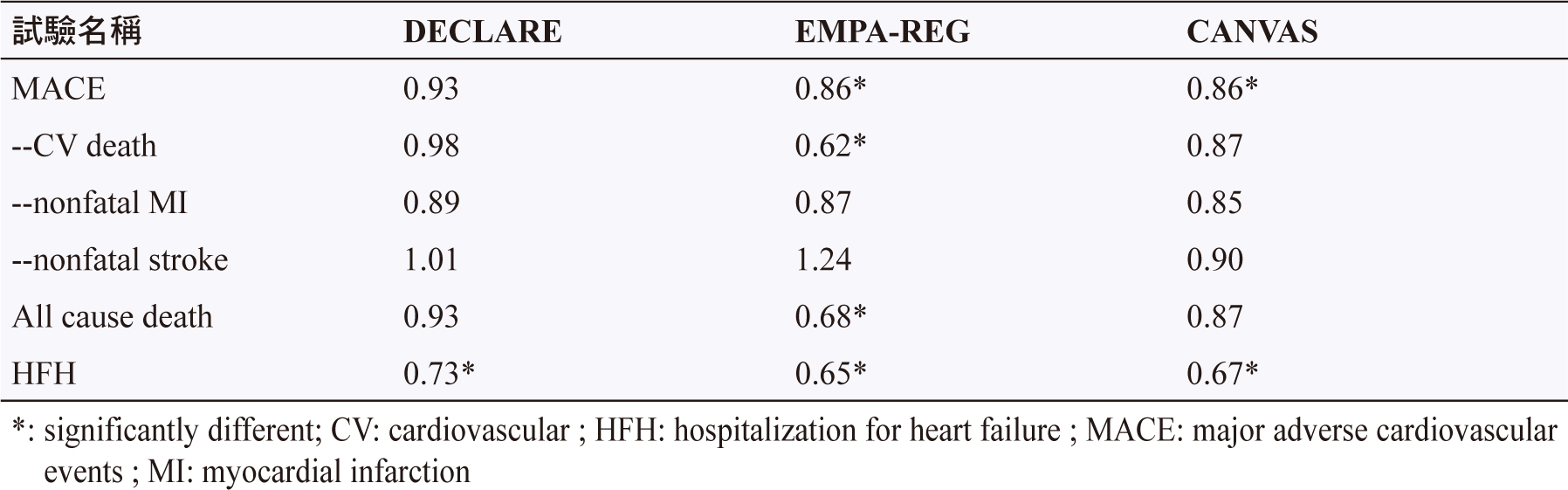
三個研究的主要試驗終點皆為 MACE,次級的心血管影響包括整體死亡風險、因心衰竭住院 (hospitalization for heart failure;HFH) 的風險等,試驗的研究結果皆以風險比 (Hazard Ratio;HR) 表示,比較內容 (表二)4-6。三個主要心血管預後 (心血管死亡,心肌梗塞,缺血性腦中風) 的合成預後,研究結果顯示 dapagliflozin 與安慰劑無差異,empagliflozin 和 canagliflozin 能降低心血管發生的風險。然而把三個拆開,僅有 empagliflozin 能降低心血管死亡的風險。再看次級試驗終點,三個研究皆可降低 HFH4-6。
表二 SGLT-2i 對心血管影響試驗的主要研究結果4-6
除了大型的隨機臨床試驗外,運用大型醫療資料庫的觀察性研究是真實世界的數據,以下比較觀察性研究的結果:
一、E Patorno 等人的回溯性研究,運用美國醫療資料庫探討 canagliflozin 與其他降血糖藥對心血管的安全性。結果顯示與其他藥物,包括 DPP-4i (dipeptidyl peptidase -4 inhibitor)、GLP-1 receptor agonist、sulfonylurea 相比,canagliflozin 顯著降低 HFH 的風險,HR 為0.70 (95% confidence interval, 0.54-0.92),發生心肌梗塞或中風的風險與其他藥物相似7。
二、OBSERVE-4D:運用4個美國醫療賠償資料庫比較 canagliflozin、其他 SGLT-2i、非 SGLT-2i 對 HFH 的影響及膝下截肢 (below-knee lower extremity;BKLE) 的風險差異。結果顯示 canagliflozin 相較於非 SGLT-2i 對 HFH 的 HR 為0.39 (95% CI, 0.26- 0.60),其他 SGLT-2i 相較於非 SGLT-2i 結果相似。對 BKLE 的 HR 為0.75 (95% CI, 0.40-1.41),未增加相關風險8。
三、CVD-REAL:運用多國 (美國、英國、瑞典、挪威和丹麥) 的醫療註冊資料庫,分別評估在有無 CVD 的病人,SGLT-2i 與其他降血糖藥物對於死亡與心臟衰竭風險的影響。結果顯示使用 SGLT-2i 對於有無 CVD 者皆降低死亡風險 (HR 皆為0.56),及降低心臟衰竭風險 (HR 分別為0.72及0.61)9。
四、CVD-REAL Nordic:運用丹麥、挪威和瑞典的醫療資料庫比較 dapagliflozin、DPP-4i 在 MACE 及其他心血管事件的影響。結果顯示與 DPP-4i 相比,dapagliflozin 在 MACE (HR 0.79, 95% CI, 0.67- 0.94)、HFH (HR 0.62, 95% CI, 0.50- 0.77)、整體死亡率 (HR 0.59, 95% CI 0.49- 0.72) 皆顯示較低風險。然而在 MI、中風、心血管死亡方面無差異10。
參、SGLT-2i 對腎臟的影響4,6,11
隨機臨床研究中設定對腎臟影響的試驗終點不同:一、DECLARE 試驗為評估腎臟的綜合症狀,包括 eGFR 超過40%降至 < 60 mL/min,發生新的末期腎病個案,腎臟引起的死亡。研究結果與安慰劑相比的 HR 為0.76 (95% CI, 0.67- 0.87)4。二、CANVAS 試驗定義為發生白蛋白尿的病程進展、eGFR 降低40%、需要腎臟替代治療 (透析或移植),因腎臟引起的死亡;白蛋白尿的病程發展的 HR 為0.73 (95% CI, 0.67-0.79),其他腎臟事件的發生 HR 為0.60 (95% CI, 0.47- 0.77)6。三、EMPA-REG 試驗為腎毒性的發生或腎臟功能惡化,包括白蛋白尿增加、血清肌酐酸上升、新增腎臟替代治療或因腎臟引起死亡事件。腎毒性的發生或腎臟功能惡化的 HR 為0.61 (95% CI, 0.53- 0.70),血清肌酐酸上升的相對風險 (relative risk;RR) 降低44%,新增腎臟替代治療的相對風險降低55%11。整體而言,研究結果顯示 SGLT-2i 可降低腎臟受損的風險。
肆、結語
隨著大型臨床試驗證實 SGLT-2i (dapagliflozin, empagliflozin, canagliflozin) 使用於第二型糖尿病療效部分可降低血糖及體重,安全性部分對心臟衰竭相關的住院率及腎臟的預後有益處,提升 SGLT-2i 在臨床的使用率。然而藥物更全面的有效性與安全性評估,尚需長久的上市後監測,佐以臨床的使用經驗。依據病人的個別性擬定治療計畫,衛教病人共同參予治療選擇與執行,觀察藥物療效,發現潛在的不良反應,以提升整體治療的成功率。
SGLT-2i, Cardiovascular and Renal Outcomes in
Type II Diabetes
Ai-Yu Yang, Chin-Feng Liu
Department of Pharmacy, Kaohsiung Medical
University Hospital,
Kaohsiung Medical University
Abstract
Type 2 diabetes mellitus is characterized by hyperglycemia, insulin resistance, and impaired insulin secretion. The goals of treatment for type 2 diabetes are to prevent or delay complications and maintain quality of life. The American Diabetes Association and the European Association for the Study of Diabetes in 2018 update the statements on the management of type 2 diabetes in adults. For patients with chronic kidney disease or heart failure and atherosclerotic cardiovascular disease, an Sodium-glucose co-transporter 2 inhibitor with proven benefit is recommended. In the randomized, double-blind trials evaluated the cardiovascular safety of the sodium‐glucose‐cotransporter‐2 (SGLT‐2) inhibitor. In patients with type 2 diabetes who had or were at risk for cardiovascular disease, treatment with empagliflozin and canagliflozin did result in a lower rate of major adverse cardiovascular events than placebo, but dapagliflozin did not significant different. And to evaluate cardiovascular outcome of real-world observational study. Diabetes is one of the risk factors for chronic kidney diseas. This article will review the cardiovascular and renal outcomes of Sodium-glucose co-transporter 2 inhibitors for the treatment of type 2 diabetes mellitus.
參考資料:
1. DeSantis A: Sodium-glucose co-transporter 2 inhibitors for the treatment of type 2 diabetes mellitus. UpToDate. Available at: https://bit.ly/2zhj0CN Accessed Nov 18, 2018.
2. Singh AK, Singh R: Recent cardiovascular outcome trials of antidiabetic drugs: A comparative analysis. Indian J Endocrinol Metab 2017;21(1):4-10.
3. Davies MJ, D'Alessio DA, Fradkin J, et al: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2018;61(12):2461-2498.
4. Wiviott SD, Raz I, Bonaca MP, et al: Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2018. doi: 10.1056/NEJMoa1812389. [Epub ahead of print]
5. Zinman B, Wanner C, Lachin JM, et al: Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015;373(22):2117-28.
6. Neal B, Perkovic V, Mahaffey KW, et al: Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes.N Engl J Med 2017;377(7):644-657.
7. Patorno E, Goldfine AB, Schneeweiss S, et al: Cardiovascular outcomes associated with canagliflozin versus other non-gliflozin antidiabetic drugs: population based cohort study. BMJ 2018;360:k119.
8. Ryan PB, Buse JB, Schuemie MJ, et al: Comparative effectiveness of canagliflozin, SGLT2 inhibitors and non-SGLT2 inhibitors on the risk of hospitalization for heart failure and amputation in patients with type 2 diabetes mellitus: A real-world meta-analysis of 4 observational databases (OBSERVE-4D). Diabetes Obes Metab 2018;20(11):2585-2597.
9. Cavender MA, Norhammar A, Birkeland KI, et al: SGLT-2 Inhibitors and Cardiovascular Risk: An Analysis of CVD-REAL. J Am Coll Cardiol 2018;71(22):2497-2506.
10. Persson F, Nyström T, Jørgensen ME, et al: Dapagliflozin is associated with lower risk of cardiovascular events and all-cause mortality in people with type 2 diabetes (CVD-REAL Nordic) when compared with dipeptidyl peptidase-4 inhibitor therapy: A multinational observational study. Diabetes Obes Metab 2018;20(2):344-351.
11. Wanner C, Inzucchi SE, Lachin JM, et al: Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med 2016;375(4):323-34.
通訊作者:楊璦瑜/通訊地址:高雄市三民區自由一路100號
服務單位:高雄醫學大學附設中和紀念醫院藥劑部藥師/聯絡電話:(O) (07)3121101 ext 7174

