摘要
自體顯性型多囊性腎臟疾病 (Autosomal Dominant Polycystic Kidney Disease; ADPKD) 是最常見的腎臟遺傳性疾病,好發於40歲成人,男性及女性罹病的機率是相同的,根據目前流行病學的研究,盛行率大約1/400到1/1000,全球病人約1200萬人。自體顯性型多囊腎病人經常會出現腎臟囊泡增大、破裂而併發腎臟囊腫感染、出血、疼痛、腎臟衰竭的情形,若不加以控制很容易進入末期腎病變的階段。在台灣,洗腎病人中約2.4%為自體顯性型多囊腎的病人,病人經常因腎臟囊泡增大、破裂而造成泌尿道感染 (urinary tract infection,UTI) 入院治療,由於 UTI 的成因可能為囊泡感染或腎臟實質發炎,因此臨床醫師在第一時間以經驗性抗生素的使用更是重要,目前許多研究在探討 fluoroquinolone 類及 trimethoprim-sulfamethoxazole 抗生素運用於此類病人感染的成效,本篇文章將深入探討治療 ADPKD 病人感染之抗生素使用。
關鍵字: 多囊腎、自體顯性型多囊性腎臟疾病、泌尿道感染、autosomal dominant polycystic kidney disease、fluoroquinolone
壹、前言
多囊性腎病 (polycystic kidney disease,PKD) 是一種遺傳性腎臟疾病,PKD 分為自體隱性型多囊性腎臟疾病 (autosomal recessive polycystic kidney disease,ARPKD) 及自體顯性型多囊性腎臟疾病 (autosomal dominant polycystic kidney disease,ADPKD),不分性別或種族其罹病率相同。世界上約有一千多萬名 PKD 病人,其中,以 ADPKD 佔大多數。根據流行病學的研究,大約每400至1000人中就會有一人患有 ADPKD,這些病人佔所有透析病人的8%至10%1。在台灣,逾7萬洗腎病人中,PKD 病人 (包含 ARPKD 及 ADPKD) 約就占5%至10%2。有30%至50%的 ADPKD 病人終其一生會經歷泌尿道感染 (urinary tract infection,UTI),經常反覆感染 UTI 更可能造成病人永久性腎損傷,因此,如何預防 ADPKD 病人 UTI 再覆發及延緩病人進展至末期腎病變,更是目前的重要議題。
貳、病因
ADPKD 病人感染 UTI 的主要細菌為格蘭氏陰性腸菌屬 (gram-negative enteric organisms),此類細菌主要來源是在急性腎盂腎炎及感染的囊泡中發現3。探究囊泡所造成的UTI,ADPKD 可分為兩個類型,包含 ADPKD1(基因遺傳變異的位置是在 chromosome 16的短臂上) 及 ADPKD2(基因遺傳變異在 chromosome 4的長臂上)。由於染色體基因的變異,因此產生多囊蛋白1(polycystin 1)及多囊蛋白2(polycystin 2)兩種細胞膜上的異常蛋白質,此異常蛋白質會使腎小管上的初級纖毛 (primary cilia) 發育不正常,一開始凸出一個囊腫,隨後持續增生形成獨立的囊體,造成腎臟囊腫不斷的產生及增大,若受感染的囊泡因不斷增大而破裂,細菌則會直接滲入膀胱系統造成 UTI4。

圖一 自體顯性型多囊腎之囊泡增生4
參、臨床表徵
臨床症狀包含:發燒、軀幹疼痛、噁心、嘔吐、少尿、頻尿、血尿。由於囊泡的周圍密布血管,血管可能因囊泡太大或其它外力而造成破裂,血液就會滲到囊泡裡造成體積變大。若持續出血,囊泡會直接破掉,血液因此會直接滲到膀胱系統而產生血尿。
肆、臨床檢驗判讀
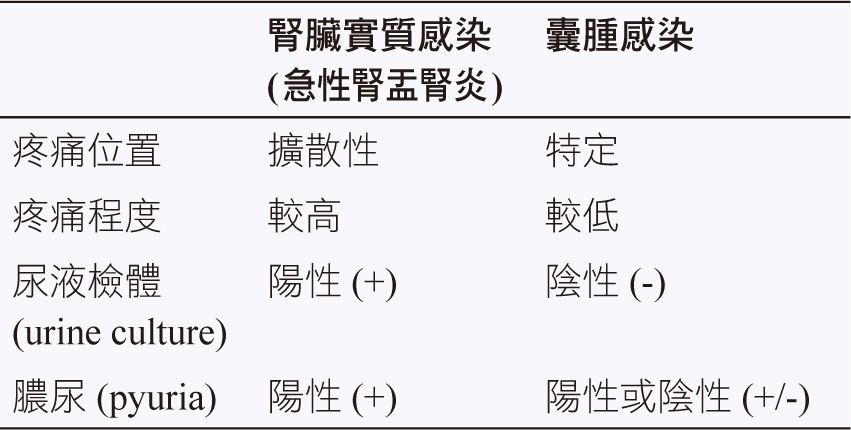
ADPKD 病人之 UTI 可能由腎臟實質感染 (急性腎盂腎炎) 或囊腫感染所造成,臨床上經常難以區別造成 UTI 之感染原因。如果是囊腫的感染,疼痛的位置比較特定、疼痛較不會嚴重、尿液檢體 (urine culture) 則因其屬於一個獨立的囊體所以通常尿液檢體是不會有任何發現 (negative),膿尿 (pyuria) 有可能是陽性 (positive) 亦可能是陰性 (negative);相對地,急性腎盂腎炎的疼痛屬於較擴散性 (diffuse),疼痛程度比起囊腫感染來的嚴重,尿液檢體多為陽性 (positive),並且會有膿尿情形 (positive) 5,6。
表一 臨床檢驗判讀
伍、治療
腎臟實質感染 (急性腎盂腎炎) 與囊泡感染所造成的 UTI 於臨床表徵上相似,而臨床醫師於最初判斷時亦難以區別,因此最初的經驗性抗生素的選擇更是重要。當懷疑是腎臟感染並且有全身性症狀入院時,應靜脈注射經驗性抗生素,而抗生素的選擇應該以能夠對抗革蘭氏陰性腸菌屬並且同時治療急性腎盂腎炎及囊泡感染為主。由於抗生素仍須能夠穿透受感染的囊泡對抗囊泡內的細菌,因此選用的抗生素包含 ciprofloxacin、levofloxacin (或其它fluoroquinolone 類) 及 trimethoprim-sulfamethoxazole。以下將分別探討各類藥物的特性7-10。
一、Fluoroquinolone
此類抗生素的作用機轉為專一性抑制細菌細胞核的去氧核糖核酸旋轉酶 (DNA gyrase;topoisomerase II) 的功能,抑制細菌 DNA 的複製及轉錄,進而殺死細菌。此類藥物能同時穿透囊泡並且為急性腎盂腎炎的首選經驗性抗生素,因此這類藥物為 ADPKD 病人併發 UTI 的首選抗生素。在臨床上治療的症狀、使用劑量、優缺點及與需要監測注意的項目 (表二)。
表二 各類抗生素之比較
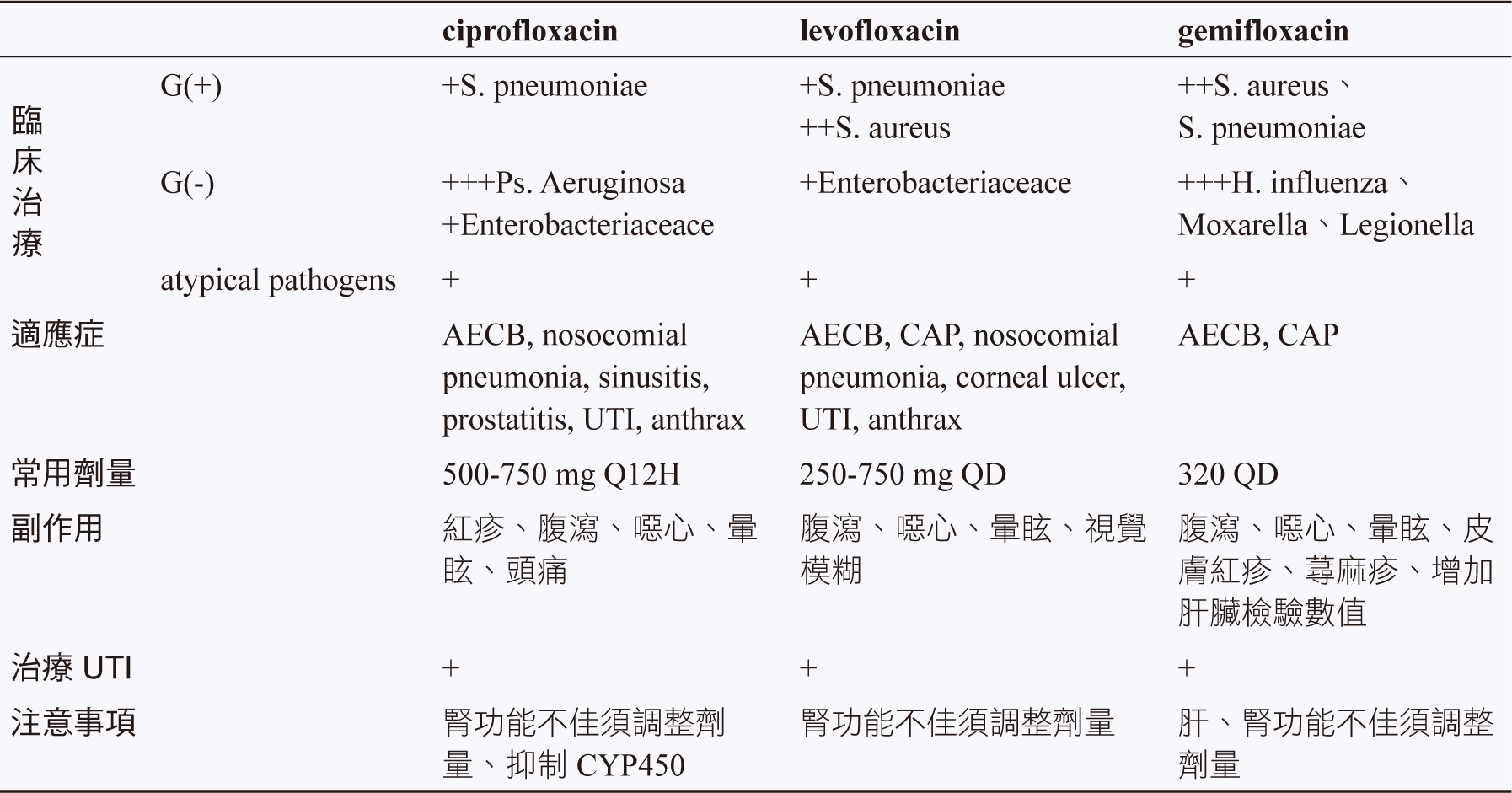
在台灣,用於全身性抗菌效果的 fluoroquinolone 包含 ciprofloxacin、levofloxacin、moxifloxacin、gemifloxacin。Moxifloxacin 因為不經過腎臟排除,不會用來治療 UTI,因此本篇不在此探討11。口服劑型的 fluoroquinolone 亦是目前對 pseudomonas aeruginosa 唯一具有抗菌效力的口服劑型抗生素,使用於 UTI 的優點除了對於整個泌尿系統皆具有良好的穿透力之外,口服劑型的 fluoroquinolone 與靜脈注射型 fluoroquinolone 皆具有相似的血清及組織濃度。
Ciprofloxacin 為第二代 fluoroquinolone 此類藥物對革蘭氏陰性菌具有殺菌力,包括hemophilus influenza、neisseria gonorrheae,特別是 pseudomonas aeruginosa 也比第三代藥物具有殺菌效力,ciprofloxacin 亦涵蓋革蘭氏陽性菌和非典型細菌 (atypical pathogens),包括legionella pneumophilia、clamydia 及 mycoplasma。此類藥物對 streptococcus pneumoniae 具有抗藥性,因此並不建議單獨使用於呼吸道感染。
Levofloxacin、gatifloxacin 為第三代的fluoroquinolone。相較於第二代,第三代的藥物具有更好的組織穿透力,而且對於非典型細菌及革蘭氏陽性菌有更好的殺菌效果,特別是 streptococcus pneumoniae,因此被歸類為 respiratory fluoroquinolone。Levofloxacin 為唯一同時對 psedomonas aeruginosa 及 streptococcus pneumoniae 具有抗菌效力的 fluoroquinolone。雖然第三代的 fluoroquinolone 對於 psedomonas aeruginosa 的效果不及第二代,但是對於其他革蘭氏陰性菌效果仍然顯著,尤其是 haemophilus influenza 及 moraxella catarrhalis。
二、Trimethoprim-sulfamethoxazole (TMP-SMX)
此類藥物之作用機轉為抑制細菌二氫葉酸還原酶 (dihydrofolate reductase, DHFR) 及二氫葉酸合成酶 (dihydropteroate synthetase,DHPS),進而抑制胸腺嘧啶 (thymidine) 合成,可抑制細菌細胞核 DNA 合成,具有殺菌作用。
由於細菌對 TMP-SMX 產生抗藥性的比例越來越高,因此目前只能用於體外抗生素試驗對於 TMP-SMX 具有敏感性的感染症。在台灣,UTI 最常見的致病菌為大腸桿菌 (Escherichia coli,E. coli),TMP-SMX對 E coli 的抗藥性約50%12。在 ADPKD 病人中,併發 UTI 的菌種亦以 E coli 為主,目前對於 ADPKD 之 UTI 抗生素治療研究甚少,但仍有文獻對於 ADPKD 併發 UTI 病人的 TMP-SMX 治療持兩面的意見。有研究指出,TMP-SMX 中的 sulfamethoxazole 無法已足夠的濃度到達遠端囊泡,因此經常造成治療上的失敗13;亦有研究指出,TMP-SMX 能有效對抗 ADPKD 併發 UTI 的菌種14,探究此篇研究,作者以七位未感染 UTI 之病人與一位感染 UTI 之 ADPKD 病人相對照,由於僅以一位感染 UTI 之病人為樣本,無法全面性應用於臨床治療上 UTI 菌種之抗藥性。因此,目前 TMP-SMX 在 ADPKD 併發 UTI 病人仍非第一線治療藥物。
陸、結論
約有30%至50%的 ADPKD 病人一生當中會經歷 UTI,致病菌以格蘭氏陰性腸菌屬所造成為主,成因通常是膀胱逆行性感染、腎結石、置放導尿管所造成。由於急性腎盂腎炎與囊泡感染所致的 UTI 最初於臨床上很難分辨,而 fluoroquinolone 類抗生素能穿透多囊腎囊泡,亦可以治療無併發症的急性腎盂腎炎。因此,建議以 fluoroquinolone 類抗生素為最初的經驗性療法。若病人確診為多囊腎囊泡感染所致則需以口服持續治療至少4週至6週。目前文獻對於 ADPKD 併發 UTI 病人以 TMP-SMX 治療持兩面的意見,因此,目前臨床上多以 fluoroquinolone 做為 UTI 的經驗性抗生素。
ADPKD 病人需要面臨長期服藥的需求及相繼而來的泌尿道感染併發症,本文探討 ADPKD 併發泌尿道感染時的抗生素治療,希望能提供臨床醫師及藥師在治療時能有更多的參考。
Treatment of UTI in ADPKD patient
Fu-Yu Yang, Wen-Jin Tung
Department of Pharmacy, Yuanlin Christian
Hospital
Abstract
Autosomal Dominant Polycystic Kidney Disease(ADPKD) is the most common hereditary renal disease. Estimated prevalence is between one in 400 and one in 1000, they often occur in fourty-years-old adaults and the morbidity rate between males and females are the same. According to the epidemiology, ADPKD affects more than 600,000 Americans and 12.4 million people worldwide.
PKD kidneys can be much larger, the size of the renal cysts can grow as large as a grapefruit, and weighing up to 30 pounds each. If the big cyst is broken, there are other symptoms that can occur in various areas of the body, such as infection, bleeding, pain, and even renal failure. The main reason of hospitalization rate is cyst broken-induced-urinary tract infection, therefore, the using of empiric antibiotics is very important in the first time. Many studies are currently investigating the efficacy of fluoroquinolone and trimethoprim-sulfamethoxazole antibiotics in the infection of such patients. This article will make a further discussion on the treatment of infection in patients with ADPKD
參考資料:
1. Polycystic kidney disease | PKD Foundation. [cited 2018 Oct 18]. Available from:https://pkdcure.org/
2. 衛生福利部國民健康署. (2016, 十二月 31).
https://www.hpa.gov.tw/Pages/List.aspx?nodeid=312
3. Sallée, M., Rafat, C., Zahar, J.-R., Paulmier, B., Grünfeld, J.-P., Knebelmann, B., & Fakhouri, F. (2009). Cyst Infections in Patients with Autosomal Dominant Polycystic Kidney Disease. Clinical Journal of the American Society of Nephrology : CJASN, 4(7), 1183-1189.
4. Happé, H., & Peters, D. J. M. (2014). Translational research in ADPKD: lessons from animal models. Nature Reviews Nephrology, 10(10), 587-601.
5. Rizk, D., & Chapman, A. B. (2003). Cystic and inherited kidney diseases. American Journal of Kidney Diseases: The Official Journal of the National Kidney Foundation, 42(6), 1305-1317.
6. Lantinga, M. A., Drenth, J. P. H., & Gevers, T. J. G. (2015). Diagnostic criteria in renal and hepatic cyst infection. Nephrology, Dialysis, Transplantation: Official Publication of the European Dialysis and Transplant Association - European Renal Association, 30(5), 744-751.
7. Schwab, S. J., Bander, S. J., & Klahr, S. (1987). Renal infection in autosomal dominant polycystic kidney disease. The American Journal of Medicine, 82(4), 714-718.
8. Bennett, W. M., Elzinga, L., Pulliam, J. P., Rashad, A. L., & Barry, J. M. (1985). Cyst fluid antibiotic concentrations in autosomal-dominant polycystic kidney disease. American Journal of Kidney Diseases: The Official Journal of the National Kidney Foundation, 6(6), 400-404.
9. Elzinga, L. W., Golper, T. A., Rashad, A. L., Carr, M. E., & Bennett, W. M. (1988). Ciprofloxacin activity in cyst fluid from polycystic kidneys. Antimicrobial Agents and Chemotherapy, 32(6), 844-847.
10. Hiyama, L., Tang, A., & Miller, L. G. (2006). Levofloxacin penetration into a renal cyst in a patient with autosomal dominant polycystic kidney disease. American Journal of Kidney Diseases: The Official Journal of the National Kidney Foundation, 47(1), e9-13.
11. UpToDate.Fluoroquinolones. : Drug information. [cited 2019 Jan 24].Available from:https://www.uptodate.com/contents/fluoroquinolones?search=fluoroquinolones&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
12. Elzinga, L. W., Golper, T. A., Rashad, A. L., Carr, M. E., & Bennett, W. M. (1987). Trimethoprim-sulfamethoxazole in cyst fluid from autosomal dominant polycystic kidneys. Kidney International, 32(6), 884-888.
13. Schwab, S. J., & Weaver, M. E. (1986). Penetration of Trimethoprim and Sulfamethoxazole Into Cysts in a Patient With Autosomal-Dominant Polycystic Kidney Disease. American Journal of Kidney Diseases, 7(5), 434-438.
14. UpToDate.Trimethoprim-sulfamethoxazole (co-trimoxazole): Drug information. [cited 2018 Jan 04].Available from:https://www.uptodate.com/contents/trimethoprim-sulfamethoxazole-co-trimoxazole-drug information.
通訊作者:楊富喻/通訊地址:彰化縣員林市莒光路456號
服務單位:員林基督教醫院藥劑課藥師/聯絡電話:(O) 04-8381456 ext 1157

