摘要
幽門螺旋桿菌 (Helicobacter pylori; H. pylori; Hp) 已證實是造成胃炎、胃及十二指腸潰瘍之原兇,更被列為胃的第一級致癌物 (WHO 1994)。以氫質子幫浦抑制劑 (proton pump inhibitor; PPI) 為基礎合併兩種抗生素的『三合一』根除療法已廣泛地被使用。然而仍有約15-20%的病人無法有效地治癒。近幾年失敗的比率正快速增加,服藥順從性及細菌本身的抗藥性是主要因素。本文希望透過實證醫學的角度,探討相對於傳統三合一療法 (amoxicillin+clarithromycin+PPI) 及使用 levofloxacin 的臨床效益比較。
關鍵字: 幽門螺旋桿菌、三合一療法、抗藥性、根除率、fluoroquinolones
壹、前言
2005年諾貝爾醫學獎得主馬歇爾 (Barry J. Marshall) 和華倫 (Robin Warren) 兩人在1982年發現幽門螺旋桿菌 (Helicobacter pylori) 是造成人類消化性潰瘍的病因。從此一連串的研究,發現感染此菌不但造成胃潰瘍、十二指腸潰瘍,且後續引發胃淋巴癌、胃癌。根據流行病學統計全球大約有50%以上的人口都曾經感染過1。在21世紀的今天,幽門螺旋桿菌的感染仍是致死的重要病原菌之ㄧ,亦是上胃腸道疾病最常見的致病因子。過去醫療界曾努力研發疫苗但未能成功:目前臨床上僅能著重於感染後的治療。但近幾年治療失敗的比率正快速增加2,本研究期望能找出有效的藥物組合,以便提高其根除率,同時避免該菌抗藥性的惡化與擴散。
貳、流行病學
在微生物學上,幽門螺旋桿菌屬於微需氧性革蘭氏陰性菌,外觀呈螺旋狀,具有鞭毛,其感染行為是以非侵入性方式寄生在宿主胃部黏膜層內,利用本身分泌之 ureas,分解 urea 產生 ammonia 來中和並防止胃酸的攻擊,故能於強酸環境下生存 (如圖一)。

圖一 H. pylori 致病機轉
流行病學的統計,全世界約有50%的人口曾感染該菌;在開發中國家更高達80%-90%,即使已開發國家如美國亦達30%~40%1。根據林肇堂先生於1993年所作的調查,在台灣地區感染率約54.4%3,感染人口推估高達一千多萬人左右。而這些受感染群也是罹患上胃腸道疾病以及「胃腺癌」及胃黏膜相關淋巴瘤 (mucosa-associated lymphoid lymphoma 簡稱 MALToma) 的高危險群4。由此可知,「幽門螺旋桿菌」的感染將會造成國人重要的健康威脅亦會導致健保龐大的費用支出。因此,對於「幽門螺旋桿菌」的根除治療是醫療與公共衛生的重要課題。
參、H. Pylori 的治療用藥現況
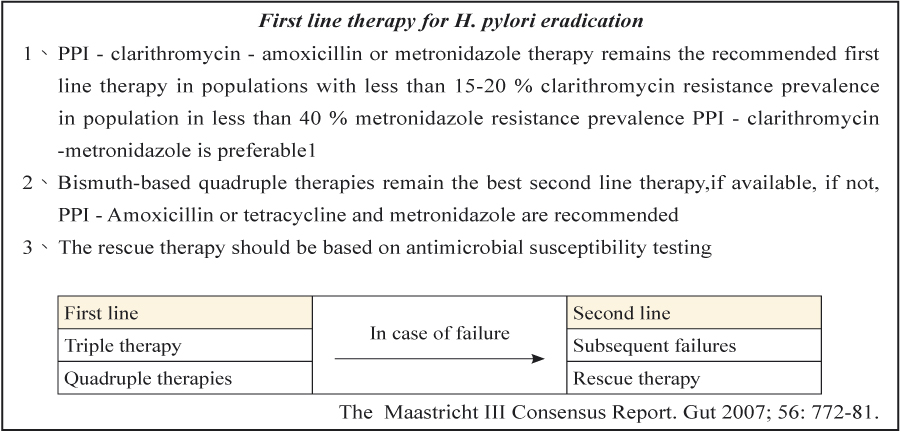
幽門螺旋桿菌可造成胃炎、胃及十二指腸潰瘍,更被列為胃的第一級致癌物。當被檢查出 H. Pylori 感染時,根除性的治療被認為重要的。而目前臨床上大多依循歐洲的第三版馬斯垂克共識 (Maastricht III consensus) (表一) 和2007年美國腸胃學會最新治療幽門螺旋桿菌的準則 (表二) 作為治療的參考;其中以氫質子幫浦抑制劑 (proton pump inhibitor; PPI) 為基礎合併兩種抗生素的三合一療法來根除 H. Pylori 為主要選擇,但這樣的治療仍有高達15-20%的病人在首次治療時失敗5。經 Hojo M 等人在2001年所作的研究中發現造成根除率失敗的主因是抗藥性6;另外根據 Graham 等人分析93位因感染 H. Pylori 治療的服藥習慣,發現如果病人服用超過處方總量60%的藥物,則Hp根除率可達96%,反之則只有69% 7。由此結果得知抗藥性與服藥遵從性是影響治療成敗的重要因素。
過去的臨床經歷以及藥物試驗,全球對於「幽門螺旋桿菌」的抗生素治療方法雖然莫衷一是,但大家都有一致性的共識,就是要使得消化性潰瘍罹患率或復發率減少,則「幽門螺旋桿菌」的根除扮演著其中很重要的角色,減少了潰瘍性疾病 (peptic ulcer disease) 再復發的機率,對於健保支出是很合乎經濟效率的。
表一 Treatment strategy
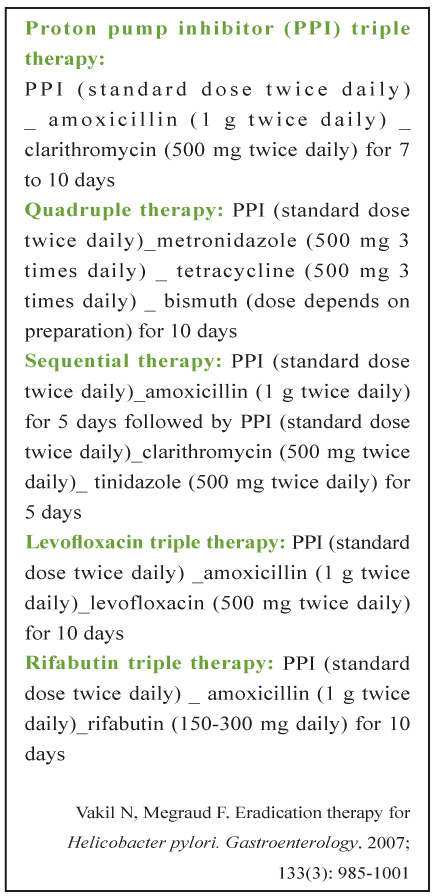
表二 Box. Treatment Regimens for Helicobacter pylori
肆、 Fluoroquinolones 與三合一療法治療幽門螺旋桿菌的成效
目前,大部份國際醫療準則仍以三合一為標準療法如表三8,9,但治療失敗卻已經變成重要的問題;而試著延長治療時間,並未顯著提高效益卻可能增加抗藥性與副作用的產生8。為了克服這些問題,選擇新的抗生素組合或簡化治療模式成為最近研究的方向。
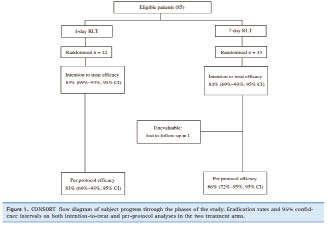
根據 E. G. Giannini et al.2006年所作的研究,共收集85名患者分成兩組,採用分析 RLT 療法 (即 ribeprazole 20 mg + levofloxacin 500 mg + tinidazole 500 mg),分別評估4天與7天的治療成效,結果顯示此種療法其根除率皆高於八成,而兩組間並無明顯差異如圖二10 ;服用天數縮短,除了增加順從性之外仍可維持治療效果。當第一線治療失敗時改用 levofloxacin,不論三合一或四合一都有不錯的成效11-13。但若因此思考 levofloxacin 成為首選藥物的可能性,就又要考慮新抗藥性產生的問題。Hung 等人於2009年調查南台灣流行率之研究中指出,fluoroquinolone 的抗藥比例雖遠低於傳統標準三合一的治療如表四14。但也強調相較於過去,不論是 ciprofloxacin 或 levofloxacint 其抗藥性從2.8% (1998-2003) 明顯增加到11.8% (2004-2007) (p =.009)。甚至 Nimish Vakil, MD et al.於 2008 American Medical Association 的討論中也提出,由於傳統療法對於 Hp 的抗藥性越來越嚴重,以二線藥物取代傳統組合無疑是根除幽門螺旋桿菌的不二策略。但不幸地,新藥之抗藥性發展亦無法避免,在近期的報告中已經限制使用 levofloxacin 作為第一線用藥。有鑑於此,Hung 等人在研究中利用 in vitro 體外分析其中12株幽門螺旋桿菌對 fluoroquinolones (FQs) 產生抗藥性的基因型態,發現 gyr A 與 gyr B 變異的基因序列相對於6種 FQs 藥物最小抑菌濃度的變化如表五,因此為了避免抗藥性一再地產生,必需朝用藥的選擇時機 (timing) 方向努力。未來如能配合檢驗技術上的進展,將會有效來選擇高敏感之抗生素發揮治療的效果。
表三 幽門螺旋桿菌的治療建議
第一線 |
一、標準三合療法: PPI 1# bid + clarithromycin 500 mg bid + amoxicillin 1 gm (或 metronidazole 500 mg) bid |
7-14天 |
二、接續性療法(Sequential Therapy): (PPI 1# bid + amoxicillin 1 gm bid) × 5天;接著再使用 (PPI 1#bid + clarithromycin 500 mg bid + amoxicillin 1 gm bid) x 5天 |
10天 |
|
三、不含鉍劑之四合一療法(Non-bismuth Containing Quadruple Therapy): PPI 1# bid + clarithromycin 500 mg bid + amoxicillin 1 gm bid + metronidazole 500 mg bid |
7天 |
|
第二線 |
一、標準四合一療法: PPI 1# bid + bismuth subcitrate 120 mg qid + metronidazole 500 mg tid + tetracycline 500 mg qid |
7-14 天 |
二、Levofloxacin為基礎之三合療法: PPI 1# bid +levofloxacin 500 mg qd + amoxicillin 1 gm bid |
7-14 天 |
|
第三線 |
一、以抗生素敏感性試驗為指引之除菌治療 |
10-14天 |
二、標準四合一療法: PPI 1# bid + bismuth subcitrate 120 mg qid + amoxicillin 500 mg qid + levofloxacin 500 mg qd |
10-14天 |
圖二 分析RLT療法 (4-day v.s 7day)
表四 In vitro activity of six antimicrobial agents against 2010 H. pylori strains isolated from 1998-2007 at National Cheng Kung University Hospital.
Ug/mL |
||||
Antibiotic |
Range |
MIC50 |
MIC90 |
Resistance (%) |
Clarithromycin |
0.03-128 |
0.03 |
0.12 |
9.5 |
Metronidazole |
0.03->256 |
2 |
>256 |
27.6 |
Tetracycline |
0.03-4 |
0.12 |
0.5 |
0.5 |
Ciprofloxacin |
0.03-32 |
0.25 |
0.5 |
5.7 |
Levofloxacin |
0.03-32 |
0.25 |
0.5 |
5.7 |
註: The resistance breakpoints for amoxicillin, clarithromycin, metronidazole, tetracycline, and fluoroquinolones were defined as ≥ 0.5, ≥ 1.0, ≥ 8, ≥ 4, and> 1.0 μg/mL, respectively. Minimal inhibitory concentrations of amoxicillin, clarithromycin, and metronidazole in H. pylori isolated from 1998–2000 were published previously and were not included in this study. |
||||
表五 Association between minimal inhibitory concentration levels and gyrA/B mutation patterns in 12 fluoroquinolone-resistant strains of H. pylori
MIC (ug/mL) |
gyrA mutation |
|||||||||
Strain no. |
Cip |
Lev |
Gar |
Gat |
Mox |
Tro |
N87 |
D91 |
Others |
gyrB mutation |
364 |
16 |
8 |
1 |
4 |
32 |
8 |
N87K |
- |
- |
A4065 |
371 |
8 |
8 |
2 |
8 |
32 |
8 |
- |
D91G |
- |
- |
409 |
16 |
8 |
1 |
8 |
32 |
8 |
- |
D91G |
- |
- |
806 |
8 |
8 |
4 |
2 |
16 |
8 |
- |
D91N |
- |
- |
917 |
16 |
4 |
1 |
2 |
8 |
4 |
- |
D91N |
- |
- |
924 |
16 |
8 |
0.5 |
2 |
8 |
2 |
- |
D91Y |
- |
- |
1022 |
8 |
2 |
0.25 |
1 |
4 |
2 |
- |
D91N |
A97V |
- |
1024 |
4 |
2 |
0.12 |
1 |
2 |
1 |
- |
D91N |
- |
- |
1026 |
32 |
16 |
4 |
16 |
32 |
16 |
N87K |
- |
H57Y |
- |
1042 |
16 |
8 |
1 |
4 |
16 |
4 |
N87K |
- |
R140K |
- |
1058 |
32 |
32 |
2 |
8 |
32 |
8 |
N87K |
- |
- |
- |
1060 |
32 |
4 |
1 |
2 |
8 |
8 |
- |
- |
- |
- |
註: Cip, ciprofloxacin; Lev, levofloxacin; Gar, garenoxacin; Gat, gatifloxacin; Mox, moxifloxacin; Tro, trovafloxacin. |
||||||||||
伍、結論
目前根除幽門螺旋桿菌失敗主要原因為服藥順應性不佳與抗藥性日益嚴重。近年來,由於廣泛使用抗生素的結果,衍生出的抗藥性,增加了藥物選擇上的困難。為了提高根除率及降低醫療支出應首重用藥順從性、病人衛教,當治療無效再考慮抗藥性問題。因此,如何找出適當的藥物組合,配合檢驗技術上的進展精準地用藥來提高治療的效果將是未來的挑戰。
參考資料:
1. Pounder RE, Ng D: The prevalence of Helicobacter pylori infection in different countries. Aliment Pharmacol Ther 1995; 9: 33-9.
2. Vakil N, Megraud F:Eradication therapy for Helicobacter pylori. Gastroenterology. 2007; 133(3): 985-1001.
3. Lin JT, Wang JT, Wang TH, et al: Helicobacter pylori infection in a randomly selected population healthy volunteers, and patients with gastric ulcer and gastric adenocarcinoma:A seroprevalence study in Taiwan . Scand J Gastroenterol 1993; 28: 1067-72.
4. Parsonnet J, Hansen S, Rondriguez L, et al:Helicobacter pylori infection and gastric lymphoma. N Engl J Med 1994; 330; 1267-71.
5. Vakil N: Primary and secondary treatment for Helicobacter pylori in the United States.Rev Gastroenterol Disord. 2005 Spring; 5(2): 67-72.
6. Hojo M, Miwa H,Nagahara A, et al: Pooled analysis on the efficacy of the second-line treatment regimens for Helicobacter pylori infection. Scand J Gastroenterol 2001 Jul; 36(7): 690-700.
7. Graham D, Low G, Malaty HM, et al: Factors influencing the eradication of Helicobacter Pylori with triple therapy. Gastroenterology 1992; 102; 493-6.
8. Fuccio L, Minardi ME, Zagari RM, et al: Meta-analysis: duration of first-line proton-pump inhibitor based triple therapy for Helicobacter pylori eradication. Ann Intern Med. 2007; 147(8): 553-562.
9. Malfertheiner P, Megraud F, O'Morain C, et al: Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut 2007; 56: 772-81.
10. E. G. Glannini, C. Bilardi, P. Dulbecco, et al: A study of 4- and 7-day triple therapy with rabeprazole, high-dose levofloxacin and tinidazole rescue treatment for Helicobacter pylori eradication. Aliment Pharmacol Ther 2006; 23: 281-287.
11. Nimish Vakil, Dino Vaira.Sequential Therapy for Helicobacter pylori: Time to Consider Making the Switch? JAMA. 2008; 300(11): 1346-1347.
12. Miehlke S, Madisch A, Bästlein E, et al: One-week triple therapy with esomeprazole, levofloxacin and amoxicillin is effective for eradication of Helicobacter pylori sensitive to metronidazole and/for clarithromycin. Helicobacter 2003; 8: 464.
13. Wong WM, Gu Q, Lam SK, et al: Randomized controlled study of rabeprazole, levofloxacin and rifabutin triple therapy vs quadruple therapy as second-line treatment for Helicobacter pylori infection. Aliment Pharmacol Ther 2003; 17: 553-560.
14. Hung KH, Sheu BS, Chang WL, et al: Prevalence of primary fluoroquinolone resistance among clinical isolates of Helicobacter pylori at a University Hospital in Southern Taiwan. Helicobacter 2009 Feb; 14(1): 61-65.
Current Treatment Regimens for Helicobacter Pylori Infection
Chien-Wen Kang, Chiu-Min Chang, Po-chang Lin
Department of Pharmacy, Madou Sinlau Christian Hospital
Abstract
Helicobacter pylori (Hp) has been confirmed that could cause gastritis, stomach and duodenal ulcer, and is listed as the first class of stomach's carcinogen (WHO 1994). Proton pump inhibitor (PPI) is the basic element to which combines two kinds of antibiotics then become as the so called triple therapy. And this way for eradicating the pathogens now is used wildly. However there still are about 15-20% patients who have failed in treatment by this Gold Rule. In recently, the ratio of treatment failure increases fast. The patients' compliance and pathogens resistance are considered the major reasons to make this condition. Based on the EBM (Evidence-Based-Medicines), the purpose of this study is to discuss the clinical benefit compared with using of levofloxacin to that of the traditional triple therapy (amoxicillin+clarithromycin+PPI).

