阿茲海默症 (Alzheimer's disease) 是老年失智症的各類型中,最普遍的一種形式。症狀來自於腦部控制思考,記憶及語言區域的神經元,產生退化性的影響。
研究指出,基因在阿茲海默症的成因中,扮演重要的角色。由阿茲海默症的遺傳原因顯示,分為兩大模式。一部分,占較少比例的突變基因,如澱粉樣蛋白前驅蛋白 (APP; amyloid precursor protein)、早蛋白一號 PSEN1 (presenilin 1) 及早蛋白二號 PSEN2 (presenilin 2),主要與小於60歲,早年家族性阿茲海默症的發生有關。另一部分,占大多數的變異基因,如E型載脂肪蛋白基因 APOE ε2 (apolipoprotein E gene 對偶ε2型) 及 APOE ε4與大於60歲,晚發性阿茲海默症的發生有關,也是一般最普遍型的阿茲海默症。
阿茲海默症是一種不可逆、進行性,神經退化性的疾病。在病人的腦中,出現不正常的瘢塊及神經纖維糾結。瘢塊主要由緻密、不可溶的澱粉樣蛋白所構成。神經糾結物主要是由於與微小管構成相關的 tau 蛋白,過度磷酸化,造成微小管扭曲變形,堆積在細胞內而產生。
新的診斷方針由美國老年研究所及美國阿茲海默症協會,召集專家團,於2011年所發表。新的方針將阿茲海默症分為三個階段:臨床前期、輕度認知障礙期和阿茲海默型失智症期。
乙醯膽鹼酯解酶抑制劑,被用來治療輕至中度阿茲海默症。幫助緩解阿茲海默症的症狀。使用的藥品有 Razadyne (galantamine),Exelon (rivastigmine),Aricept (donepezil) 及 Cognex (tacrine)。Namenda (memantine) 是一種 NMDA (N-methyl-D-aspartate) 受體拮抗劑,用來治療中度至重度的阿茲海默症,主要的效果為延遲阿茲海默症的進展。
新的診斷及治療模式,正在浮現,來自於對阿茲海默症的病程及病理的了解。在未來,可能對於50歲以上的族群,進行風險評估,以便及早辨別發生阿茲海默症的機率及預防。
關鍵字:阿茲海默症、β澱粉樣蛋白、濤蛋白、乙醯膽鹼酯解酶抑制劑、NMDA 受體拮抗劑
壹、前言
愛羅斯.阿茲海默 (Alois Alzheimer),一位德國精神病學家,於1907年發表了「老年癡呆症」的病例。之後此一類型的病人,便以阿茲海默症 (Alzheimer's disease; AD) 為名。主要的症狀有,健忘、記憶喪失,隨著病情加重,失去語言及空間辨別的能力,最終失去日常生活能力而死亡,是一種腦神經退化的病症。在近期阿茲海默症的研究上1,基因有很大的影響力。因此又可以分為:
一、 家族性阿茲海默症 (Familial AD; FAD)
發生於60歲前,與家族遺傳有關,占整體 AD 的5%,重要的影響基因有 APP、PSEN1、PSEN2。
二、 阿茲海默老年失智症 (Senile dementia with Alzheimer's type; SDAT)
發生於60歲後,占阿茲海默症的大多數,影響的基因在 APOEε4及 APOEε2,在阿茲海默症的病程上,確診的前8年,病人的認知功能就會下降,確診後的存活期約7年,是一種慢性不可逆的退化性疾病。
貳、流行病學
阿茲海默症好發於60歲以上的老人,年齡是危險因子。然而年輕人亦有可能得到阿茲海默症。據估計2,有500萬的美國人,患有阿茲海默症。65-74歲的男性與女姓,有5%患有此病,超過65歲的老人,每增加5歲,患病人數約會增加一倍。因此預估,超過85歲以上的老人,將有一半患有阿茲海默症。目前,阿茲海默症是美國成年人前十大死因第6位,65歲以上的老人死因的第5位。自1980年以來,美國患病的人數已翻倍,預估到了2050年,約有1600萬人,罹患此病。在醫療保險的支出上,患有阿茲海默症及失智症的患者,是未患病者的3倍。
參、病理學
在研究阿茲海默症的神經病理學上3,發現患者的腦組織切片,出現老年斑塊 (senile plaques) 及神經纖維糾結 (neurofibrillary tangles) 的現象。更進一步分析斑塊的成份,為β型澱粉樣蛋白 (β-amyloid peptide; Aβ) 的沉積物。目前研究認為,過度β型澱粉樣蛋白沉積,會引起腦神經一連串的生化反應,進而引起神經細胞壞死。腦神經細胞的壞死,是產生阿茲海默症的症狀原因。但是,究竟是何種原因,造成β型澱粉樣蛋白過度沉積,目前還在研究當中。在已知的原因裡,遺傳基因,是一重要因素。β型澱粉樣蛋白的上游來源為澱粉樣蛋白前驅物 (amyloid precursor protein) (APP),是一種一次穿膜蛋白,廣範的分佈在細胞膜上。在正常的酵素切割下,下游的產物,可以作為細胞內的傳訊分子。當酵素切割產生變易,造成β-secretase 活性增加,將會造成下游產物β型澱粉樣蛋白大量生成,進而導致β型澱粉樣蛋白的堆積。過度堆積的β型澱粉樣蛋白,會引起神經中的免疫細胞-微小膠細胞 (microglia) 活化,及傳訊調節細胞-星狀細胞 (astrocyte) 活化,引發過度發炎的反應,最終使神經細胞凋亡 (apoptosis)。在發炎反應中,會使與神經微小管構造相關的濤蛋白 (tau protein) 過度磷酸化,引發微小管的變型糾結。因此,過度發炎的反應是引起神經壞死及變形的原因 (圖一)3。
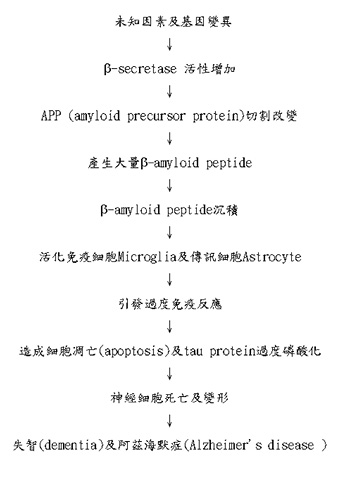
圖一 阿茲海默症的可能成因3
肆、阿茲海默症的診斷
阿茲海默症是失智症 (dementia) 中的一種。根據美國精神科協會所發表的精神疾病診斷標準手冊第四版 (DSM-IV),所定義的失智症標準為4:一、出現記憶力喪失或減退的症狀。二、同時合併出現右列至少一項症狀 (一)失語症 (aphasia) (二)失用症 (apraxia) (三)失認症 (agnosia) (四)執行能力異常 (impair executive function)。三、有以上認知功能障礙並導致職業及社交功能的影響,並排除有譫妄 (Delirium) 的情形。
診斷阿茲海默症還需搭配醫師作智能測驗 MMSE (mini mental state test) 及腦部斷層掃描作判斷。
美國老年研究所 (National Institute on Aging; NIA) 及美國阿茲海默症協會 (Alzheimer's Association),在2011年,公布了新版阿茲海默症的診斷定義5,6,做為確立病程及研究方向。將阿茲海默症,細分為三個階段7:(一)臨床前期:腦部發生改變,有澱粉樣蛋白堆積,神經細胞改變,但無明顯症狀出現。(二)輕度認知障礙期 (mild cognitive impairment;MCI):有記憶及思考障礙,相較於正常年齡及教育狀況的人群,但不影響生活的獨立性,可能或不可能,繼續發展成阿茲海默型失智症 (Alzheimer's dementia)。(三)阿茲海默型失智症期:出現阿茲海默症的症狀,包括記憶喪失、用詞困難、視覺及空間定向能力混亂,損壞個人生活的獨立性。
新的準則,建議生化檢查 (biomarks)8,以確立阿茲海默症的診斷,包含核磁共振成像 (magnetic resonance imaging;MRI),正子攝影 (positron emission tomography;PET),腦脊髓液 (cerebrospinal fluid;CSF) 蛋白檢測。
伍、阿茲海默症的藥物治療
現今阿茲海默症的藥物治療9,只能減輕病情的症狀,減緩病程的進展,並不能達到治癒的目標。藥物的使用,分為兩階段。
一、治療輕至中度的阿茲海默症
在腦中,乙醯膽鹼 (acetylcholine),是重要的神經元傳訊的分子,影響記憶功能。因此,提升腦神經中乙醯膽鹼的量,有助於失智的緩解。目前是使用乙醯膽鹼酯解酶抑制劑 (cholinesterase inhibitor) 藥品,減緩乙醯膽鹼的分解。美國 FDA 核準的藥品,包含(一)Razadyne (galantamine) (二)Exelon (rivastigmine) (三)Aricept (donepezil) (四)Cognex (tacrine)。Cognex 由於副作用較大,已少使用。這些藥品,皆為乙醯膽鹼酯解酶抑制劑,並沒有明確文獻指出,何種最有效。但在不同病人的選用上,不同病人,有最適切的選擇 (表一)。
表一 阿茲海默症使用藥品9
藥名 |
藥品類型及使用 |
藥物作用 |
常見副作用 |
建議劑量 |
Namenda (memantine) |
NMDA antagonist 治療中度至重度阿茲海默症 |
抑制 glutamate 作用及活性 |
頭暈、頭痛、便秘、認知困惑 |
錠劑:起始劑量5 mg/day 於一週內調整至最大劑量20 mg/day 以內 溶液劑型:同錠劑 長效劑型:起始劑量7 mg/day 於一週內調整至最大劑量28 mg/day 以內 |
Razadyne (galantamine) |
Cholinesterase inhibitor 治療輕度至中度阿茲海默症 |
抑制 acetylcholine分解 刺激 nicotinic receptor 並促進 acetylcholine 在腦中釋放 |
噁心、嘔吐、腹瀉、體重下降、胃口差
|
錠劑:起始劑量8 mg/day 於四週內調整至最大劑量24 mg/day 以內 溶液劑型:同錠劑 長效劑型:同錠劑但一天一次 |
Exelon (rivastigmine) |
Cholinesterase inhibitor 治療輕度至中度阿茲海默症 |
抑制 acetylcholine及 butyrylcholine 在腦神經分解
|
噁心、嘔吐、腹瀉、體重下降、胃口差、肌肉無力
|
膠囊:起始劑量3 mg/day 於二週內調整至最大劑量12 mg/day 以內 溶液劑型:同錠劑 長效劑型:同錠劑但一天一次 貼片:起始劑量4.6 mg/day 於四週內調整至最大劑量13.3 mg/day 以內 溶液劑型:同膠囊 |
Aricept (donepezil) |
Cholinesterase inhibitor 治療輕度至中度阿茲海默症 |
抑制 acetylcholine在腦神經分解
|
噁心、嘔吐、腹瀉 |
錠劑:起始劑量5 mg/day 於三個月內調整至最大劑量23 mg/day 以內 |
Cognex (tacrine) |
Cholinesterase inhibitor 治療輕度至中度阿茲海默症 |
抑制 acetylcholine在腦神經分解 |
噁心、反胃、嘔吐、腹瀉、發抖、皮疹 |
起始劑量40 mg/day 於四週內調整至最大劑量80 mg/day |
二、治療中度到嚴重阿茲海默症
阿茲海默症為退化性的腦神經疾病,如何減緩神經細胞死亡,是治療方式之一。Glutamate 是興奮性的胺基酸,透過活化腦中 NMDA 受體 (N-methyl D-aspartate receptor) 達到興奮神經元的作用。過度興奮的神經元,會導致神經元死亡。因此,選用藥品 Namenda (memantine) ,一種 NMDA 受體拮抗劑 (NMDA receptor antagonist),達到阻斷興奮效果。使用 Namenda 有延緩病程,增加病人正常生活品質時間的效果。
陸、討論
在未來,新的診斷及治療模式正在形成3。對於50歲以上的族群,提供有效的罹病風險評估,並針對高危險族群,作預防性治療。
在阿茲海默症的預防上,檢測是重要方式,有助於病程的控制。方向有:一、高危險族群基因檢測。二、腦成像攝影技術,諸如核磁共振成像 (magnetic resonance imaging;MRI),正子攝影 (positron emission tomography;PET) 等。三、生化數值 (biomakers) 檢測,諸如腦脊髓液中Aβ42,濤蛋白 (tau protein)濃度及血液中Aβ濃度的測定。
在阿茲海默症的治療上,如何發展出有效的治療藥物,是重要的目標。目前由於在致病的機轉上,已較過去清晰,因此在新藥物的研究上,有較明確的方向。
新的方向有:一、γ-secretase inhibitors:在β澱粉樣蛋白的形成上,γ-secretase是重要的切割酵素,抑制γ-secretase將減少β澱粉樣蛋白的形成。二、抗聚合化合物 (anti-aggregating compound):β澱粉樣蛋白的形成,是從簡單的單體到複雜的聚合物,使用抗聚合化合物,將減少沉積物的形成。三、抗發炎藥品:在阿茲海默症的病程上,神經元過度發炎,最終導致神經元死亡。使用新的抗神經元發炎藥品,有助於延緩病程。四、使用抗氧化藥品:在神經元發炎過程中,氧化性自由基過多,將導致細胞傷害。使用抗氧化藥品,有助於減少細胞損傷及死亡。
透過檢測能力的加強及新藥的開發,將有助於阿茲海默症整體的預防及治療的進步。
The Etiology and Treatments of Alzheimer’s Disease
Yu-Zhe Yang, Cheng-Chou Sun
Department of Pharmacy, Kang-Ning General Hospital
Abstract
Alzheimer's disease is the most common form of dementia among older adults. The disease involves parts of the brain that control thoughts, memory, and language.
Studies indicate that genetic factors are estimated to play an important role in Alzheimer's disease. The inheritance of Alzheimer's disease exhibits a dichotomous pattern. On one hand, rare mutations of genes in APP, PSEN1, and PSEN2 are fully penetrating for early-onset (< 60 years) familial Alzheimer's disease, On the other hand, common gene polymorphisms, such as the genes of APOEε2 and APOEε4 for common late-onset Alzheimer's disease.
Alzheimer's disease is a irreversible, progressive, neurodegenerative disease where the brain develops abnormal plaques and neurofibrillary tangles. Plaques are dense, mostly insoluble deposits of -amyloid peptide. Tangles are aggregates of microtubule-associated protein tau which has become hyperphosphorylated and accumulated inside the cells.
The new diagnostic guidelines for Alzheimer's disease developed by expert panels convened by the National Institute on Aging (NIA) and Alzheimer's Association in 2011. The new guidelines focus on three stages of Alzheimer's disease: preclinical Alzheimer's, mild cognitive impairment (MCI) due to Alzheimer's, and dementia due to Alzheimer's.
Cholinesterase inhibitors are prescribed for mild to moderate Alzheimer's disease. These drugs may help delay or prevent symptoms from becoming worse for limited times and may help control behavioral symptoms. The medications include Razadyne (galantamine), Exelon (rivastigmine), Aricept (donepezil), and Cognex (tacrine). Namenda (memantine), an N-methyl D-aspartate (NMDA) antagonist, is prescribed to treat moderate to severe Alzheimer's disease. The main effect is to delay progression of the symptoms of Alzheimer's.
A new diagnostic and treatment paradigm is emerging from the more understanding of the disease cascade. In the future, it is likely that individuals reaching older than 50s or beyond will be offered a specific risk-assessment profile to determine their likelihood of developing Alzheimer's disease.
參考資料:
1. Tanzi RE: A brief history of Alzheimer's disease gene discovery. J Alzheimers Dis. 2013;33 suppl 1:s5-13.
2. Centers for Disease Control and Prevention: Alzheimer's Disease. (accessed at http://www.cdc.gov/aging/aginginfo/alzheimers.htm)
3. Dennis J, Selkoe: Alzheimer's disease: Genes, Proteins, and Therapy. Physiol Rev 2001;vol 81 no.2:741-766.
4. American Psychiatric Association: Diagnostic criteria for Dementia of the Alzheimer's Type. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. (accessed at http://www.behavenet.com/node/21508)
5. McKhann GM, Knopman DS, Chertkow H, et al: The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011 May;7(3):263-269.
6. Hyman BT, Phelps CH, Beach TG, et al: National Institute on Aging-Alzheimer's Association guidelines for the neuropathologic assessment of Alzheimer's disease. Alzheimers Dement. 2012;8(1):1-13.
7. Alzheimer's disease education and referral center: Diagnostic guidelines for Alzheimer's disease: frequently asked questions for clinicians. (accessed at http://www.nia.nih.gov/alzheimers/diagnostic-guidelines-alzheimers-disease-frequently-asked-questions-clinicians)
8. Alzheimer's Association: New Diagnostic Criteria and Guidelines for Alzheimer's disease. (accessed at http://www.alz.org/research/diagnostic_criteria/#top)
9. Alzheimer's disease education and referral center: Alzheimer's Disease Medications Fact Sheet. (accessed at http://www.nia.nih.gov/alzheimers/publication/alzheimers-disease-medications-fact-sheet)

