摘要
目標:研究透過醫院資訊系統 (hospital information system, HIS) 降低老年患者使用潛在不適當用藥 (potentially inappropriate medications, PIMs) 之成效。
方法:本研究共分為兩階段,第一階段評估2011年10月至12月間年齡大於或等於65歲且長期使用藥物 (處方天數 ≧ 28天) 的患者所使用的藥品,以2012 AGS Beers Criteria 列舉「須避免使用的藥物」為依據,找出研究對象最常使用的 PIMs。CSPIMs (Chung Shan PIMs) 為本院醫師、藥師組成之專家團隊所定義本院不建議老年患者使用之 PIMs,並於2013年1月1日起開始透過 HIS 警示;第二階段評估2013年1月至3月間 HIS 介入後研究對象 CSPIMs 的使用情況。
結果:在第一階段12,237名研究對象中,有4,437名患者 (36.2%) 所服用的藥品至少有一種或一種以上是 PIM,包含 zolpidem (23.7%)、dipyridamole (20.5%) 與 glyburide (15.7%) 等共計49項藥品,經專家團隊定義12項藥品為 CSPIMs 並於 HIS 系統設定警示。排除第二階段未繼續領藥之病人,本研究共追蹤9,062老年患者,平均年齡75.5 ± 6.5歲,其中男性佔44.6%。HIS 警示介入前,有2,660名 (29.4%) 老年患者使用了3,288個 CSPIMs;HIS 警示介入後,服用藥品中有 CSPIMs 的患者減少為1,645名 (18.2%, p < 0.001),平均每位患者減少使用0.12個 CSPIMs (p < 0.001),其中以 estazolam、lorazepam 和 clonazepam 三種藥品使用病人數減少最多。
結論:透過 HIS 之 CSPIMs 警示,可明顯減少長期服用藥品的老年患者使用 CSPIMs。
關鍵字: 潛在性不適當用藥、醫療資訊系統、老年患者、potentially inappropriate medications、hospital information system、elderly patient
壹、前言
眾多研究顯示,避免使用潛在性不適當用藥 (potentially inappropriate medications, PIMs),可降低用藥問題的產生1。PIM 定義為已知有更有效、副作用較低的藥物時,仍給予易引起藥物不良反應、藥物毒性等高風險的用藥來治療疾病2,Beers Criteria 明確地列舉老年患者使用哪些藥物為 PIMs;在2012年時由美國老年醫學會 (The American Geriatrics Society, AGS) 主導更新了藥物以符合目前臨床的使用狀況,也提昇了偵測 PIMs 的敏感度3,因此新版本的 Beers Criteria 又稱為2012 AGS Beers Criteria4。
過去研究顯示,約有四分之一到醫院求診的老年患者所領取的藥品中,有一種以上的 PIMs5;本土研究更顯示,在2001-2004間有六成老年患者的處方中,有一種以上的用藥是 PIMs6,足見老年患者使用PIMs的比例甚高,用藥安全已亮起紅燈,本研究希望透過醫院資訊系統 (hospital information system,HIS) 之介入,減少老年患者使用 PIMs,增加老年患者用藥安全。
貳、研究對象與方法
本研究共分為兩階段,第一階段為回溯型的世代研究 (retrospective cohort study),即利用本院之「藥局作業系統」收集2011年10至12月間門診病人的就醫紀錄,僅將年齡 ≧ 65歲、長期使用藥物 (處方天數 ≧ 28天) 的12,237名患者納入研究中;研究期間患者所領用的藥物若與前次相同時,則僅評估第一次領取藥品,而若病人同時領用其他長期處方,則一併納入分析。所使用藥物以2012 AGS Beers Criteria 列舉「須避免使用的藥物」為依據,了解這群患者最常使用 PIMs,參照80/20法則由醫師、藥師共同討論,針對第一階段使用頻率高且容易導致嚴重藥物事件的藥品,定義本院不建議老年患者使用之 PIMs 為 CSPIMs,並於 HIS 中設定 CSPIMs 警示,即當醫師開立這些藥品給年齡 ≧ 65歲且處方天數 ≧ 28天的門診病人時,則會跳出 CSPIMs 警示視窗,警示內容為該藥不建議使用之適應症或可能引發之藥物不良事件 (圖一),介入時間為2013年1月1日起;第二階段為前瞻性世代研究 (prospective cohort study),分析 HIS 介入後研究對象2013年1月至3月期間是否再使用 CSPIMs,排除條件為此段期間未繼續領藥的患者,藉以評估醫師對於 CSPIMs 警示的接受情況。將以卡方與 t 檢定分別確認 HIS 介入後患者是否有服用 CSPIMs 與平均每位患者服用 CSPIMs 之項數的成果,統計分析採雙尾檢定,若p值小於0.05則視為具有統計上顯著意義。本研究通過本院人體試驗委員會審核 (案號為 CS12117)。
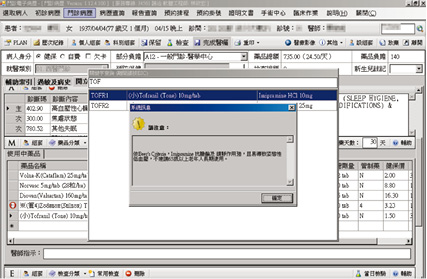
圖一 HIS 中設定 CSPIM 警示視窗
參、結果
第一階段研究期間 (2011年10至12月),長期使用藥物 (醫師處方 ≧ 28天) 的老年患者(年齡 ≧ 65歲) 合計12,237名,最常使用的 PIMs 包括 zolpidem、dipyridamole 與 glyburide 等。
經醫師、藥師共同討論並於 HIS 系統設定警示共計12項 CSPIMs (表一);排除2013年1月至3月期間未來領藥之患者3,175人,完成一、二階段的研究對象共計9,062人,平均年齡75.5 ± 6.5歲,其中男性佔44.6%。平均每位病人之疾病診斷數為4.9 ± 2.7,服用藥品種類為5.2 ± 2.7種。CSPIMs 警示介入前,9,062人中有2,660名 (29.4%) 老年患者使用藥品至少有一種或以上是 CSPIMs,12項 CSPIMs 共處方3,288次;CSPIMs 警示介入後,減少為1,645名病人使用 CSPIMs,盛行率降為18.2% (p < 0.001),12項 CSPIMs 處方減少為1,833次,平均每位患者減少使用0.12個 CSPIMs (p < 0.001),各 CSPIMs 警示醫師接受度如圖二表示,其中以 estazolam、clonazepam 與 lorazepam 等藥品下降最多。
表一 於 HIS 中設定為 CSPIM 之藥品及警示內容
藥品 |
系統警示內容 |
Estazolam |
避免用以老年人失眠,情緒激動或譫妄之治療 |
Clonazepam |
避免用以老年人失眠,情緒激動或譫妄之治療 |
Lorazepam 0.5 & 1 mg |
避免用以老年人失眠,情緒激動或譫妄之治療 |
Amiodarone |
針對老年人,速率控制較節律控制有較好的臨床效益 |
Quetiapine 25 & 100 mg |
避免用以治療失智症患者的行為異常 |
Propafenone |
針對老年人,速率控制較節律控制有較好的臨床效益 |
Dihydroergotoxine |
療效不明確 |
Trihexyphenidyl |
針對帕金森氏症有更有效的藥品選擇 |
Imipramine |
抗膽鹼及鎮靜作用強,且易導致姿態性低血壓 |
Zolpidem |
易導致跌倒,避免長期使用 (超過90天) |
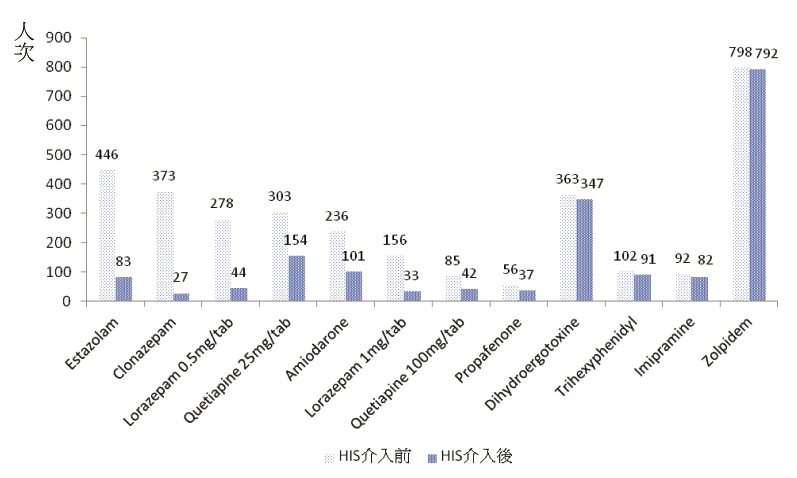
圖二 各CSPIM 於 HIS 警示前後使用人次之比較
肆、討論
第一階段研究期間約有36.2%長期用藥的老年患者所服用的藥品中至少一種或一種以上為2012 AGS Beers Criteria 列舉的 PIMs,與過去在台灣門診 PIMs 盛行率的研究10.5%至23.7%7-9比較起來,本院的盛行率明顯偏高,雖然與研究對象疾病嚴重度及使用不同的評估準則有關,但如何避免老年患者使用 PIMs,仍是刻不容緩的課題。而大家都知道在醫療資訊系統中建構過多的警示等於沒有警示,本研究將參照80/20法則,故召集專家 (包含醫師、藥師) 針對第一階段使用頻率高且使用該藥易引發藥物不良事件的藥品定義本院老年患者不建議使用之 CSPIMs,而考量到有不少品項為含 glyburide 之複方藥品,且 glyburide 主要處方科別為新陳代謝科,醫師們表示很清楚 glyburide 藥理特性僅開立給必須使用的患者,另外2012 AGS Beers Criteria 雖然指出使用 dipyridamole 會增加老年患者姿勢性低血壓的風險,但證據等級僅有中等,為避免影響醫師看診流暢度,因此本研究並未將 glyburide、dipyridamole 列入 CSPIMs 中。
本院透過 HIS 之 CSPIMs 警示,提醒醫師所處方的藥品中包含 CSPIMs,請醫師再審慎評估藥品使用的必要性或考慮替換其他較安全或有效的藥品。在連續追蹤三個月後,研究對象使用 CSPIMs 的盛行率由29.4% 降至18.2%,顯示透過 HIS 之 CSPIMs 警示的確是降低老年患者使用 CSPIMs 的有效方式,之中成效最佳者為 estazolam、clonazepam 與 lorazepam 等藥品,可見多數醫師認同老年患者長期使用 benzodiazepines 類藥品易引起跌倒、意識不清等藥物事件,經警示後便鮮少用於失眠,情緒激動或譫妄之治療。而 zolpidem 與 dihydroergotoxine 為警示後使用量大且接受度較低的兩項藥品,分析主因為 zolpidem 警示內容為「易導致跌倒,避免長期使用 (超過90天)」,醫師們認為未將 zolpidem 處方於慢性處方箋便忽略了 HIS 的警示,使得 zolpidem 在 HIS 介入前後使用人次無太大變化;目前警示方式已修改為醫師開立處方後,累計使用 zolpidem 的天數超過90日的處方。至於 dihydroergotoxine 雖文獻證實「療效不明確」,但醫師表示臨床使用病人反應良好,且未產生藥物不良事件,故在警示後仍選擇繼續使用。經與院內專家們討論後,目前已將 dihydroergotoxine 排除於 CSPIMs 之外。
伍、結論
研究結果顯示透過 HIS 之 CSPIMs 警示可明顯減少老年患者使用 CSPIMs,特別是 benzodiazepines 類藥品接受度最高,顯見醫師亦認同使用此類藥品易引起老年患者跌倒、意識不清等藥物不良事件;而經醫師評估後仍處方 CSPIMs 的病人,可透過藥師加強衛教,使其了解服藥時該注意的事項、可能不良反應發生狀況及相關處理原則,以有效提升老年患者用藥安全。
陸、誌謝
感謝本院提供專題研究計畫經費補助 (CSH-2013-A-008)。
Decreasing the Use of Potentially Inappropriate Medications among Elderly Patients
Huei-Chao Lee1, Po-Yu Chi1, Shu-Ling Tzeng2, Min-Ling Tsai3, Shiuan-Chih Chen3
Department of Pharmacy, Chung Shan Medical University Hospital1
Institute of Medicine, Chung Shan Medical University2
School of Medicine, Chung Shan Medical University3
Abstract
Objective: To determine the effectiveness of interventions by hospital information system (HIS) to decrease the use of potentially inappropriate medications (PIMs) among elderly patients.
Methods: The study is divided into two stages; the first stage of the study is to detect which PIMs have always been prescribed in elderly patients (≧ 65 years) with long-term prescription (≧ 28 days) during October to December 2011. PIMs were assessed according to "medications to avoid in older adults" listing in 2012 Beers criteria. CSPIMs were PIMs defined by the expert panel members (e.g., geriatric medicine and pharmacy practice) which medications are suggested not to be prescribed among elderly patients in our hospital. Second stage of the study is to find out the change in usage of CSPIMs of cohort during January to March 2013 after intervention by HIS.
Results: Among 12,237 patients in first stage of study, 4,437 (36.2%) patients were prescribed with at least ≧ 1 PIMs. There are 49 kinds of PIMs including zolpidem (23.7%), dipyridamole (20.5%), glyburide (15.7%), etc. There are 12 kinds of CSPIMs selected by expert panel members and were set interventions in HIS. Excluded patients who did not refill their prescriptions, there are 9,062 elderly patients included in the cohort; the mean age of the patients was 75.5±6.5 years and 44.6% were males. Before interventions of HIS, 2,660 elderly patients (29.4%) received 3,288 CSPIMs. After interventions of HIS, the number of elderly patients who take CSPIMs was declined to 1,645 (18.2%, p < 0.001), the average of received CSPIMs by each patient decreased to 0.12 (p < 0.001). The top three CSPIMs reduced in the number of patients are estazolam, lorazepam and clonazepam.
Conclusions: Interventions by HIS do reduce prescribing CSPIMs among elderly patients who taking medicines for a long time.
參考資料:
1. Gurwitz JH, Field TS, Harrold LR, et al: Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA 2003;289:1107-16.
2. Beers MH, Ouslander JG, Rollingher I, et al: Explicit criteria for determining inappropriate medication use in nursing home residents. Arch Intern Med 1991;151:1825-32.
3. Undela K, Bansal D, D'Cruz S, et al: Prevalence and determinants of use of potentially inappropriate medications in elderly inpatients: A prospective study in a tertiary healthcare setting. Geriatr Gerontol Int 2013 May 6. doi: 10.1111/ggi.12081.
4. Anonymous: American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012;60:616-31.
5. Scott IA, Gray LC, Martin JH, et al: Minimizing Inappropriate Medications in Older Populations: A Ten-step Conceptual Framework. Am J Med 2012;125:529-37.
6. Lai HY, Hwang SJ, Chen YC, et al: Prevalence of the prescribing of potentially inappropriate medications at ambulatory care visits by elderly patients covered by the Taiwanese National Health Insurance program. Clin Ther 2009;31:1859-70.
7. Lin HY, Liao CC, Cheng SH, et al: Association of potentially inappropriate medication use with adverse outcomes in ambulatory elderly patients with chronic diseases: experience in a Taiwanese medical setting. Drugs Aging 2008;25:49-59.
8. 李國任、陳俊傑、顧明祥等:老年慢性病門診病人之潛在性不適當處方的相關危險因子探討。臺灣家庭醫學雜誌2012; 22: 187-97。
9. Chang CM, Liu PY, Yang YH, et al: Potentially inappropriate drug prescribing among first-visit elderly outpatients in Taiwan. Pharmacotherapy 2004; 24:848-55.

