摘要
Ceftriaxone 所引起之藥物過敏反應 (Drug-related rash with eosinophilia and systemic symptoms, DRESS) 症候群是一種罕見且可能危及生命之藥物過敏性反應。疾病特性潛伏期長約2-6週,儘管停用可疑藥品後因為發作期長故有復發的可能性,其復發頻率與一種潛在性人類皰疹病毒之再活化有關。在一篇前瞻性研究中顯示其年發病率為0.9/100,0001。初始症狀為皮膚發疹並可能擴展至全身,亦可能同時伴隨發燒、淋巴結腫大及肝、腎、肺臟等器官發炎,以及血液異常 (包括嗜伊紅性白血球增加、非典型淋巴球增生) 等症狀。
本案例為一位25歲男性因心內膜炎而使用 ceftriaxone,於治療後發現病人產生藥物不良反應 (DRESS),本文主要探討個案發生 DRESS 後的臨床症狀與後續處置狀況。
關鍵字:ceftriaxone、Drug-related rash with eosinophilia and systemic symptoms (DRESS)
壹、前言
一、Ceftriaxone 簡介
Ceftriaxone 屬於第三代頭孢菌素類抗生素,可被用來作為心內膜炎治療,針對葡萄球菌、鏈球菌、肺炎雙球菌、腦膜炎球菌及其他具有感受性細菌引起之感染症皆具有顯著之治療效果,靜脈給藥後能夠分佈至全身,包括發炎的腦脊髓液,嚴重的藥物過敏反應和血液學異常極為少見,其他有被報導過的藥物不良反應包括:蕁麻疹、皮疹、腹瀉、嘔吐、暫時性嗜中性白血球減少、溶血性貧血2。
二、 Ceftriaxone 所引起 DRESS 臨床症狀
DRESS 是一種影響皮膚及全身多器官的嚴重過敏性疾病,約有80%為藥物所引起,其死亡率則高達10%,主要的死亡原因包括急性肝衰竭、多器官衰竭、猛爆性心肌炎3,4。常見發生於使用抗癲癇藥物、dapsone、allopurinol (表一),少數使用乙內醯胺類抗生素 (β-lactam) 也曾被報導,其中,又以 lamotrigine 在孩童的發生率為最高1/1005,6。在疾病初期患者可能發生高燒 (38-40℃)、全身無力、瀰漫性淋巴結腫大和皮疹,依疾病的進展,患者臉部、上半身以及四肢皮膚會出現紅疹,像麻疹樣迅速蔓延、融合形成紅斑或伴隨出現臉部水腫、紅斑浸潤、脫落性皮膚炎和紫癜7。另外高達50-90%的患者可能出現白血球增多症伴隨嗜伊紅性白血球 > 700/μL;30-70%的患者可能出現非典型淋巴細胞增多;80%的患者血清丙氨酸轉氨酶 (ALT) 大於正常值的二倍3,4。大約九成的病人至少一個身體器官受到侵犯,包括肝臟 (60-80%)、腎臟 (10-30%)、肺臟 (5-25%)3。文獻中指出某些病人可能因為使用 allopurinol 而引起急性間質性腎炎8。另外,在患者的支氣管肺泡灌洗液中可能發現具藥物特異性 CD8+ T 淋巴細胞和嗜酸性白血球細胞9。疾病確診也可以經由皮膚切片、貼布試驗呈陽性 (positive patch tests) 或體外試驗 (例如淋巴細胞增殖試驗) 得到進一步支持10。
表一 造成 DRESS 相關的藥物

貳、案例報告
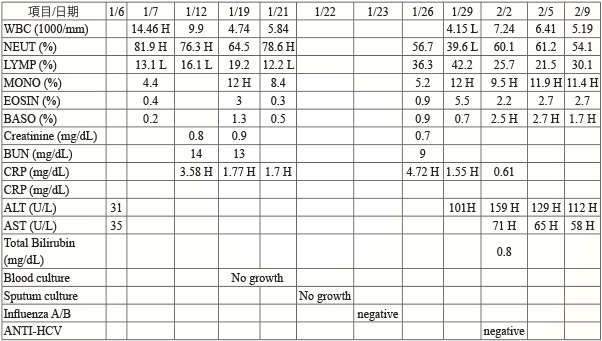
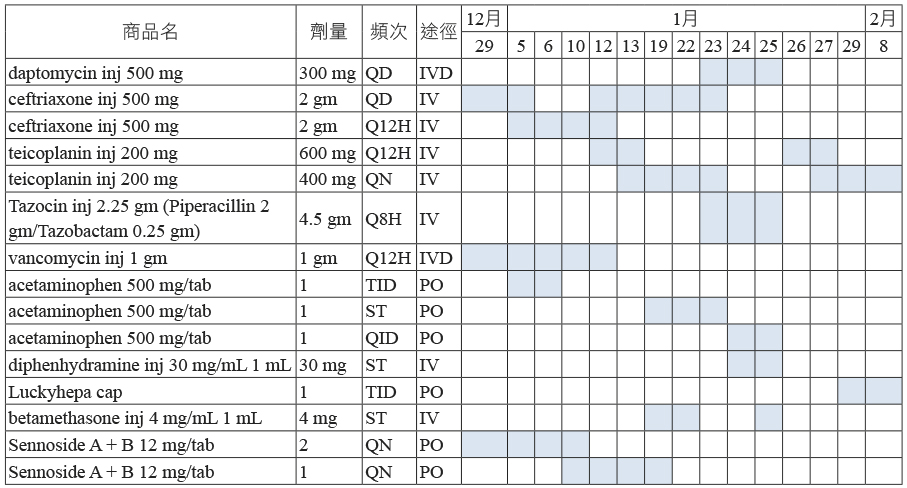
一位25歲男性病人,被懷疑為心內膜炎感染,經由醫師診斷入院接受治療。患者從103/12/29開始使用 ceftriaxone (500 mg/vial) 4/qd IV,104/01/05增加劑量為 (500 mg/vial) 4/q12h IV,在104/01/12-104/01/23改為 (500 mg/vial) 4/qd IV。103/12/30 HSV IgM: positive、EBV-VCA IgM: positive、mycoplasma P. Ab: negative、chlamydia Ag: negative、RPR : non-reactive、CMV (PCR): negative、P. jirovecii (PCR): negative。
104/01/19病人出現高燒達39.4度以及前胸、後背紅疹但不會癢,故醫師開立 acetaminophen (500 mg/tab)/q4hprn、betamethasone inj (4 mg/amp)/stat IV 緩解症狀。104/01/23病人左側頸部淋巴結腫大且發燒症狀一直存在 (圖一),醫師將 ceftriaxone 停用,改用 Tazocin (2.25 gm/vial) 2/q8h IV、daptomycin (500 mg/vial) 300 mg/qd IV 治療原來的疾病,於104/01/25病人再次出現前胸、後背及上肢紅疹,分佈範圍超過49%體表面積、高燒達39.4度,醫師開立 acetaminophen (500 mg/tab)/stat、betamethasone inj (4 mg/amp)/stat IV、diphenhydramine (30 mg/amp)/stat IV、normal saline 500 mL (3bot) qd IV 治療並且停用 Tazocin。104/01/19 以及104/01/21 blood culture no growth、104/01/23 influenza A/B screen : negative。
104/01/26皮膚紅疹消失但是左側頸部淋巴結腫大仍然存在,104/01/29肝指數出現異常 ALT 101U/L,醫師開立 Luckyhepa 1cap tid 治療,於104/3/3追蹤降至25 U/L。104/02/02 anti-HCV: negative (表二、表三)。
表二 病人住院期間的檢驗報告
表三 病人住院期間的用藥紀錄
參、討論
一、Ceftriaxone 引起 DRESS 之分析
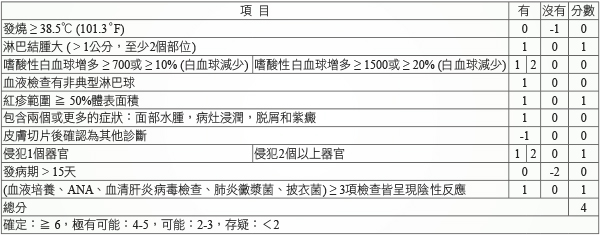
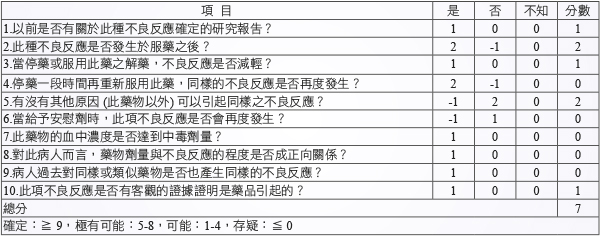
個案從使用 ceftriaxone 第22天開始出現 DRESS 症狀,這些反應牽涉到具藥物特異性的T細胞,屬於遲發型藥物過敏反應。另外,人類疱疹病毒的活化,也可能在 DRESS 症候群發病之前或病程中扮演重要的角色,特別是 HHV-611。對於無法確診或排除病人是 DRESS,根據多種臨床評估工具,包括 Bocquet et al. criteria、RegiSCAR criteria、Japanese consensus group criteria,其中以 RegiSCAR 評分表最常被用來診斷 DRESS12。本案例以 RegiSCAR 以及 Naranjo 評估表,對 ceftriaxone 引起 DRESS 進行相關性評估後 (表四、表五),皆顯示該藥品極有可能 (得分分別為4分/7分) 是引起 DRESS 之藥物。
表四 Ceftriaxone 之 RegiSCAR 評估表
表五 Ceftriaxone 之 Naranjo 評估表
二、臨床症狀與處置
在確定可疑的藥物後應即時停用,治療期間也應該避免再使用類似藥品。某些出現脫落性皮膚炎症狀的病人,則需要進一步體液、電解質以及營養的補充,額外的處置包含需要一個溫暖濕潤的環境以及溫和的皮膚照護 (溫水浴/濕敷)7。對於腎臟或肺臟沒有顯著臨床症狀以及實驗室影像學變化,僅肝臟轉氨酶輕微升高者,只要對症治療即可。另皮膚搔癢和發炎反應,則建議使用高效能的外用皮質類固醇製劑連續使用一週來緩解13。有嚴重肝臟細胞損傷的病人,可能需要做肝臟移植;有肺部呼吸困難、胸部影像學檢查異常、低血氧或血清肌酸酐值超過正常的150%、有蛋白尿或血尿的病人,建議使用中高效能的全身性皮質類固醇來治療。Prednisolone 0.5-2 mg/kg per day 持續使用直到症狀獲得改善,之後,逐步調降維持劑量治療8-12週7。此個案發生藥物不良反應之前持續使用超過兩週以上的藥品僅有 ceftriaxone,治療劑量皆在合理範圍內,於用藥期間未曾使用中草藥物或保健食品,且無潛在的藥品交互作用存在;在104/01/23停用 ceftriaxone 後,於104/01/25個案再度出現高燒皮膚紅疹情形,疑似使用 Tazocin (β-lactam) 後再次引起的過敏反應,104/01/25停用 Tazocin;104/01/29出現肝臟轉氨酶 ALT 101U/L 異常,此藥物不良反應應與 DRESS 之延遲性反應有關。
三、DRESS 的預後
個案出院後於門診追蹤期間肝指數已恢復到正常值。多數病人在停藥後數週至數月疾病會完全恢復。在一篇回溯性研究報告指出,少數病人在不良反應痊癒後約數月或數年可能發生自體免疫性疾病,包括葛瑞夫茲氏症、自體免疫性溶血性貧血14。另外,對於曾經發生過 DRESS 的病人,在最初的幾個月裡復發的可能性相當高,如果病人在更早之前曾服用過同樣的藥物,則發病時間會縮短,有報告指出這可能與 HHV-6病毒活化有關11。雖然文獻指出只有少數的病人會因為服用可疑的藥物而導致 DRESS 的發生,然而發生 DRESS 後所造成的死亡率達5-10%,應不容忽視。
肆、結論
本文希望藉由此個案報告,能讓所有醫療人員提高警覺,當患者出現皮疹、高燒、不正常的血液檢查或臟器損傷等症狀,能立即評估可能引起的原因。越早停止使用可疑的藥物,則病人的預後越好。如果是因為藥物過敏而造成的,患者應被告知,避免進一步的接觸。
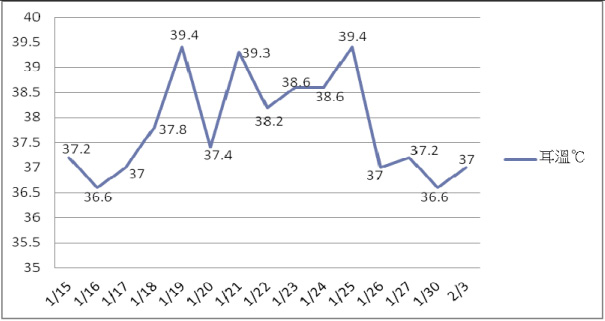
圖一 住院期間的體溫變化
A Case Report of Ceftriaxone Induced Drug Related Rash with Eosinophilia and Systemic Symptoms
Sheng-Ru Lin, Bai-Yin Tsao, I-Hsun Li, Cheng-Chih Hsieh
Department of Pharmacy, Tri-Service General Hospital
Abstract
Drug-induced Drug-related rash with eosinophilia and systemic symptoms (DRESS) is a rare, potentially life-threatening, drug-induced hypersensitivity reaction. DRESS is characterized by a long latency (two to six weeks) between drug exposure and disease onset, a prolonged course with frequent relapses despite the discontinuation of the culprit drug, and frequent association with the reactivation of a latent human herpesvirus infection. In a prospective study shows that annual incidence of 0.9/100,0001. Drug-induced hypersensitivity reaction that includes skin eruption, fever, lymphadenopathy ,internal organ involvement (liver, kidney, lung) inflammation and hematologic abnormalities (eosinophilia, atypical lymphocytosis).
This article will discuss a 25 year-old male patient with endocarditis after taking ceftriaxone cause severe adverse drug reactions (DRESS). Also, it will include patient clinical feature, medical treatment.
參考資料:
1.Muller P, Dubreil P, Mahé A, et al: Drug Hypersensitivity Syndrome in a West-Indian population. Eur J Dermatol 2003; 13: 478.
2. Akcam FZ, Aygun FO, Akkaya VB: DRESS like severe drug rash with eosinophilia, atypic lymphocytosis and fever secondary to ceftriaxone. Journal of Infection 2006; 53: 51-53.
3. Kardaun SH, Sekula P, Valeyrie-Allanore L, et al: Drug reaction with eosinophilia and systemic symptoms (DRESS): an original multisystem adverse drug reaction. Results from the prospective RegiSCAR study. Br J Dermatol 2013; 169: 1071.
4. Cacoub P, Musette P, Descamps V, et al: The DRESS syndrome: a literature review. Am J Med 2011; 124: 588.
5. Tennis P, Stern RS. Risk of serious cutaneous disorders after initiation of use of phenytoin, carbamazepine, or sodium valproate: a record linkage study. Neurology 1997; 49: 542.
6. Guberman AH, Besag FM, Brodie MJ, et al: Lamotrigine-associated rash: risk/benefit considerations in adults and children. Epilepsia 1999; 40: 985.
7. Roujeau JC: Drug reaction with eosinophilia and systemic symptoms (DRESS). UpToDate online. Available at http://www.uptodate.com.(cited:05/06/2015)
8. Chen YC, Chiu HC, Chu CY. Drug reaction with eosinophilia and systemic symptoms: a retrospective study of 60 cases. Arch Dermatol 2010; 146: 1373.
9. Guillon JM, Joly P, Autran B, et al: Minocycline-induced cell-mediated hypersensitivity pneumonitis. Ann Intern Med 1992; 117: 476.
10. Cabanas R, Prior N, Bobolea ID et al: Use of the Lymphocyte Transformation Test in the Diagnosis of DRESS Syndrome Induced by Ceftriaxone and Piperacillin-tazobactam:Two Case Reports. J Investig Allergol Clin Immunol 2010; 20: 433-436.
11. Tohyama M, Hashimoto K, Yasukawa M, et al: Association of human herpesvirus 6 reactivation with the flaring and severity of drug-induced hypersensitivity syndrome. Br J Dermatol 2007; 157: 934.
12. Guleria VS, Dhillon M, Gill S,et al: Ceftriaxone induced drug rash with eosinophilia and systemic symptoms. J Res Pharm Pract. 2014; 3: 72-74.
13. Uhara H, Saiki M, Kawachi S, et al: Clinical course of drug-induced hypersensitivity syndrome treated without systemic corticosteroids. J Eur Acad Dermatol Venereol 2013; 27: 722.
14. Chen YC, Chang CY, Cho YT, et al: Long-term sequelae of drug reaction with eosinophilia and systemic symptoms: a retrospective cohort study from Taiwan. J Am Acad Dermatol 2013; 68:459.

