摘要
背景:美國腸胃科醫學會建議,經內視鏡檢查後判定為高風險潰瘍出血患者,應給予高劑量連續輸注質子幫浦阻斷劑 (proton pump inhibitors, PPIs),但陸續有統合分析文獻與學會建議有所分歧,認為不論是否為高風險潰瘍出血患者,給予非高劑量 PPIs (QD/Q12 h) 其預後不劣於高劑量連續輸注 PPIs。本研究目的在了解院內潰瘍性出血患者 PPIs 使用情形並分析其預後。
方法:回溯性研究搜集本院2013年1月至2014年12月期間,經診斷疾病碼 ICD 9為531.4-533.9、578.9之消化性潰瘍相關疾病,且接受內視鏡止血治療後之患者,使用連續輸注 PPIs 與間歇式 PPIs 兩組之一、住院天數、二、累計紅血球輸血量 (packed red blood cells, PRBCs)、三、死亡率進行數據統計,分析兩組之預後。
結果:2013-2014年度共收錄103人,給予連續輸注 PPIs 共77人,間歇性 PPIs 共26人。兩組效果成效的測量指標為累計輸血量、住院天數與死亡率,其 p value 分別為0.976,0.744,0.365,均不具統計上差異;納入患者依出血風險高低進行相關係數 (Correlation coefficient, r) 分析,其結果為無論高風險或低風險出血性潰瘍患者,以高劑量連續輸注或非高劑量 PPIs 兩種不同方式投藥,對於住院天數、輸血量與死亡率,均不具顯著相關性。
結論:出血性潰瘍患者經內視鏡止血治療後,給予連續輸注 PPIs 並未獲得更好的預後,以經濟層面考量應使用間歇性 PPIs。
關鍵字:質子幫浦阻斷劑、proton pump inhibitors、bleeding peptic ulcer、intermittent proton pump inhibitors、continuous proton pump inhibitors
壹、前言
消化性潰瘍出血 (Peptic ulcer bleeding) 為常見就醫及住院原因,其高發病率、高死亡率的特性,造成龐大的醫療費用支出,因此如何有效預防再出血為治療重要目標。
消化性潰瘍出血常見的原因為:一、消化性潰瘍,二、糜爛性胃炎,三、食道或胃靜脈瘤,四、食道胃接合處黏膜撕裂,其中消化性潰瘍為最常見的原因。
消化性潰瘍為食道、胃、十二指腸等之黏膜受到胃液之侵蝕而形成之深入組織的消化道壁良性破損,潰瘍發生在胃為胃潰瘍,發生在十二指腸即為十二指腸潰瘍。通常消化性潰瘍是指胃或十二指腸潰瘍,僅有少數潰瘍會發生在食道。
一、消化性潰瘍出血症狀
約有75%患者之出血部位於上消化道,最常見的症狀為吐鮮血或咖啡渣樣的嘔吐物以及解黑便或柏油樣瀝青便。黑便的成因為血紅素經腸內細菌分解後,轉變成血黑素所致;當病人解出鮮紅或暗紅色血便時,大部分來自下消化道出血,但也有10%左右嚴重的上消化道出血也會解出血便。
二、消化性潰瘍風險評估量表
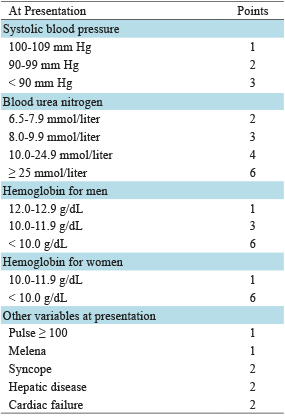
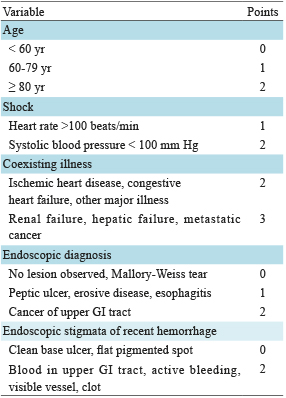
針對消化性潰瘍出血患者,需評估其預後分數,分辨風險高低並給予相對應之治療。Rockall score 和 Blatchford score 為兩種常見用於消化性潰瘍之風險評估量表,Rockall score 主要依據年齡、有無休克、共病症 (comorbidity)、還包括胃鏡檢查之發現;Blatchford score 未納入年齡而多考量了尿素值和血紅素,相較 Rockall score,較著重於臨床症狀 (表一、表二)1。
表一 Blatchford core1
表二 Rockall score1
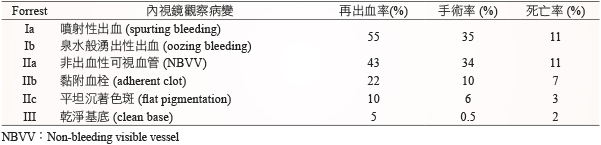
臨床表徵為評估潰瘍性出血的重要依據,而內視鏡檢查 (esophagogastroduodenoscopy) 可提供更確切的預後訊息,從內視鏡依觀察潰瘍類型分級,其再出血率、需手術介入率及死亡率有所差異 (表三)2,分類包括活動性出血:Ia 噴射性出血 (spurting bleeding) 和 Ib 泉水般湧出性出血 (oozing bleeding);IIa 露出血管,但已呈凝血狀態 (non-bleeding visible vessel),IIb 已止血狀態的黏附性血栓 (adherent clot),IIc 呈紅色、褐色或黑色沉著色斑 (flat pigmentation);III 乾淨基底 (clean base)。Ia、Ib、IIa、IIb 其再出血率或需介入率較高,為高風險潰瘍出血類型,IIc 和 III 則為低風險潰瘍出血類型。
表三 Forrest 分級表
三、消化性潰瘍治療
大多數消化性潰瘍出血患者經治療可獲相當的療效,包括及時補充輸液、給予制酸劑、治療性內視鏡和手術。治療性內視鏡可快速鑑別患者潰瘍出血嚴重程度並有效降低再出血率、減少手術介入和死亡率,內視鏡治療的止血成功率很高,但仍有15-20%患者會發生再出血 (rebleeding),而90%的再出血發生在止血後72小時內3,因此內視鏡治療後給予藥物穩定血塊以預防再出血發生是相當重要的。質子幫浦阻斷劑 (proton pump inhibitors, PPIs) 可提升胃內 pH 值,穩定血塊而達到較佳預後。
2012年美國腸胃科醫學會 (American College of Gastroenterology) 建議4,經內視鏡檢查後判定為高風險潰瘍出血患者,包括活動性出血、非出血性可視血管與具黏附血栓,給予 PPIs 80 mg IV bolus 後應以高劑量連續 (continuous) 輸注 PPIs 72小時 (輸注速率為8 mg/hr) 預防再次出血,本文簡稱此給藥方式為「高劑量 PPIs」;而間歇性給藥方式 (QD/Q12h) 則簡稱為「非高劑量 PPIs」。
回溯過去文獻,2007年香港國際內視鏡研討會發表一項隨機分派試驗,入院後48小時經內視鏡止血後,隨機分派至非高劑量 (40 mg QD) 或高劑量 omeprazole 兩組,高劑量 omeprazole 組別有較低再出血率 (3% v.s 16%),但此結果統計學上並無差異5,此試驗受試者僅61人可能使最終統計結果偏移;資料庫 UpToDate 提及指引建議於高出血風險潰瘍患者使用高劑量連續輸注 PPIs,但2014年統合分析指出經過內視鏡治療後,以非高劑量給予 PPIs 患者於臨床上多項臨床指標均不劣於高劑量 PPIs 組別,包括再出血率、PRBCs 累積輸血量與死亡率6;甚至表示非高劑量 PPIs 具有較低再出血風險傾向。以上文獻均為隨機分派試驗,本研究搜集某醫學中心之消化性潰瘍患者進行病例對照研究 (case control study),以了解高劑量 PPIs 治療消化性潰瘍患者相較非高劑量 PPIs 於臨床上之預後。
貳、材料與方法
本研究搜集本院2013年01月01日起至2014年12月31日止,經診斷疾病碼 ICD 9為531.4-533.9,578.9之消化性潰瘍相關疾病且接受內視鏡治療後患者,針對使用高劑量或非高劑量 PPIs (Pantoprazole、esomeprazole) 兩組之1.住院天數、2.PRBCs 累計輸血量、3.死亡率進行數據統計,分析兩組之預後。
個案資料收集依照病歷記載,患者需於當次就診接受內視鏡治療之後,使用 PPIs 才可納入本研究,所有分析以p值小於0.05方有統計意義,在基準點的比較上連續變數獨立以 t-test 檢定,類別變數則以 X2-test 檢定,相關係數以 Correlation coefficient, r檢定,統計分析以 SPSS 第14版分析。
參、結果
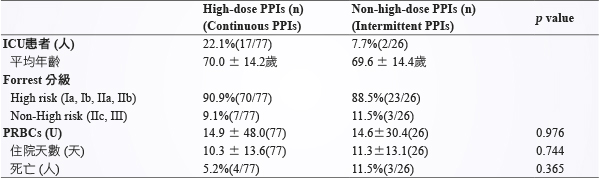
2013-2014年共收錄103人 (表四),使用高劑量 PPIs 共77人,平均年齡70.0歲,非高劑量 PPIs 共26人,平均年齡69.6歲,高劑量 PPIs 組別中 ICU 患者佔22.1%,非高劑 PPIs組別中 ICU 患者佔7.7%。兩組效果成效的測量指標為 PRBCs、住院天數與死亡率,其 p value 分別為0.976,0.744,0.365,均不具統計差異,高劑量 PPIs 組並未比非高劑量 PPIs 組獲得較好的預後,兩組之間的 PRBCs、住院天數與死亡率均無統計上差異。
表四 2013-2014年院內收集統計結果
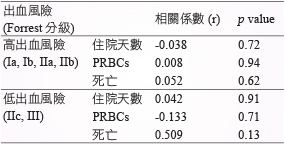
根據 Forrest 分級將個案依出血風險進行相關係數 (Correlation coefficient, r) 分析 (表五),無論是高風險或非高風險出血患者,以高劑量 PPIs 或非高劑量 PPIs 兩種不同方式投藥,對於住院天數、輸血量與死亡率並無顯著相關性。
表五 依出血風險,持續性或間歇性輸注方式投予 PPIs 與住院天數、PRBCs、死亡之相關性
肆、討論
體外試驗結果指出,胃內 pH 6以上可穩定血塊7,理論上高劑量連續輸注 PPIs 應能更有效維持此標準以防止再出血發生,腸胃科醫學會也有此建議,但近年來統合分析整合各試驗的結果顯示,以非高劑量給予 PPIs 其預後不劣於高劑量連續輸注 PPIs 組別,其中台大團隊針對高風險消化性潰瘍出血患者進行統合分析8,結果顯示高劑量連續輸注 PPIs 無法更進一步改善患者預後,包括再出血率、外科手術率或死亡率;回溯性分析本院消化性潰瘍出血患者使用 PPIs 情形也與文獻獲得相同結果,無論是否為高出血風險患者,使用較高成本之高劑量 PPIs 病人並未減少住院天數和累積輸血量,而在不良反應方面,有文獻指出長期使用 PPIs 可能會造成骨折與困難梭狀芽孢桿菌 (Clostridium difficile) 相關腹瀉風險增加9,10,主要由於抑制胃酸的分泌的影響,造成腸內的細菌異常增生而導致腹瀉,骨折風險增加原因不明;目前雖無輸注高劑量 PPIs 之不良反應之文獻,但相較非高劑量 PPIs 其相對副作用增加是很有可能的,若能使用非高劑量 PPIs 可能降低病人之副作用,並減少資源與藥費浪費,以更經濟實惠的方式達到相同之療效。
Analysis of Proton Pump Inhibitors Therapy for Peptic Bleeding Ulcers
Ya-Lan Chang1, Lei-Yu Chang1, Ya-Ju Chuang1, Chung-Hung Tsai2, Chien-Ying Lee3
Department of Pharmacy1, Institute of Medicine, Chung Shan Medical University2,
Department of Pharmacology, Chung Shan Medical University3
Abstract
Backgroud: Recommendations from American college of gastroenterology indicated that patients with high-risk bleeding ulcer based on endoscopy should be administered with high-dose continuous infusion of proton pump inhibitor (PPI). Different opinion from meta-analysis studies expressed that whether patients with high-risk bleeding ulcer, the prognosis of administered with non-high dose intermittent PPI therapy (QD / Q12 h) is not inferior to high-dose continuous infusion of PPI therapy. The purpose of this study is to investigate the usage of PPI in patients with bleeding ulcer in hospital and analyze the prognosis.
Method: We performed a retrospective study from 2013 to 2014 in our hospital. ICD-9-CM diagnosis codes of peptic ulcer-related diseases were 531.4 -533.9 and 578.9, endoscopic hemostasis performed in these patients after treatment. To compare the outcomes between high-dose continuous infusion PPI therapy with non-high dose intermittent PPI therapy, including the hospital length of stay, transfusion of packed red blood cells (PRBCs) and mortality. To compare the prognosis in these two groups from statistical analysis.
Results: This study enrolled 103 patients, 77 patients administrated with high dose continuous infusion PPI therapy, 26 patients administrated with non-high dose intermittent PPI therapy. There were no significant differences between two study groups in any of hospital length of stay, transfusion of PRBCs and mortality. (respectively, p value 0.976, 0.744, 0.365). Furthermore, we analyzed the correlation of coefficient (r) in patients divided into high and low bleeding risk. Comparison between high-dose PPI therapy with non-high dose PPI therapy, there was no significant correlation between two groups in hospital length of stay, transfusion of PRBCs and mortality.
Conclusion: Patients with bleeding ulcer after endoscopic hemostasis, administrated with high dose continuous infusion PPI therapy did not get better prognosis, intermittent PPI therapy was recommended when considering with economic aspects.
參考資料:
1.Gralnek IM, Barkun AN: Management of Acute Bleeding from a Peptic Ulcer.N Engl J Med 2008;359:928-37.
2. Laine L, Peterson WL: Bleeding peptic ulcer. N Engl J Med 1994;331:717-27.
3. Leontiadis GI, Sharma VK: Proton pump inhibitor treatment for acute peptic ulcer bleeding. Cochrane Database Syst Rev. 2006;1(1):CD002094.
4. Laine L, Jensen DM. Management of patients with ulcer bleeding. Am J Gastroenterol. 2012;107 (3):345-61.
5. Chan WH, Khin LW, Chung YF, et al: Randomized controlled trial of standard versus high-dose intravenous omeprazole after endoscopic therapy in high-risk patients with acute peptic ulcer bleeding. Br J Surg. 2011;98(5):640-44.
6. Hamita Sachar, Keta Vaidya: Intermittent vs Continuous Proton Pump Inhibitor Therapy for High-Risk Bleeding Ulcers A Systematic Review and Meta-analysis. JAMA Intern Med. 014;174(11):1755-62.
7. Chaimoff C, Creter D, D:The effect of pH on platelet and coagulation factor activities. Am J Surg. 1978;136(2):257-259.
8. Chih-Hung Wang, Matthew Huei-Ming Ma, Hao-Chang Chou, et al: High-Dose vs Non-High-Dose Proton Pump Inhibitors After Endoscopic Treatment in Patients With Bleeding Peptic Ulcer. Arch Intern Med. 2010 May;170(9):751-758
9. Yu EW, Blackwell T, Ensrud KE, et al: Acid-suppressive medications and risk of bone loss and fracture in older adults. Calcif Tissue Int 2008; 83: 251-9.
10. Howell MD, Novack V, Grgurich P, et al: Iatrogenic gastric acid suppression and the risk of nosocomial Clostridium difficile infection. Arch Intern Med 2010; 170: 784-90.

