摘要
壓瘡是組織受到無法緩解的壓迫發生損傷所造成的病變。除了讓病人受苦外,壓瘡也會延長住院天數與增加照護費用。目前對於第一期與第二期壓瘡使用親水性膠體敷料即有效。
Phenytoin 是一個抗癲癇藥物,其齒齦增生的副作用被認為是癒合傷口的一個契機。Phenytoin 涉及多個癒合過程,譬如增加膠原與其他結締組織、降低細菌污染與滲出液的量。外敷 phenytoin 在第三期與第四期壓瘡會較有治療角色存在。因為全身吸收性小,使用外敷 phenytoin 時未見一般口服 phenytoin 的副作用。因為溶解度低與 PH 值高,使用 phenytoin 的錠劑、膠囊及注射劑型於外敷可能會造成刺痛與灼熱感,然而病人可能因為痛覺受器已受損所以不覺那麼疼痛。對於適當的外敷劑量與研發劑型仍需要進一步的臨床研究做確認。
關鍵字: pressure ulcer、bedsore、decubitus ulcer、wound healing、phenytoin
壹、前言
壓瘡 (pressure ulcers) 又稱為褥瘡 (bed sores),是臥床病人常見的照護問題;若控制不佳可能會引發敗血症、延長住院與醫療成本增加。而 phenytoin 此抗癲癇藥有一齒齦增生 (gingival hyperplasia) 的副作用;有研究因此發想 phenytoin 有促進傷口癒合的潛能1,2。醫學發展日新月異,藥物的潛能也漸漸被開發;好比有醫師會嚐試 theophylline 拉高心跳,原本不討喜的副作用或許是治療另一個疾病的新契機。
貳、流行病學
壓瘡在不同的照護機構有不同的盛行率:於急性醫院為3-17%3,於護理之家為10-35%4。
參、壓瘡的病理機制
形成壓瘡的過程牽涉很多因素,可大類分為外力 (external forces) 與病人本身的因素 (host factors)。單單只是外力像是剪力 (如不正確拖拉病人) 或摩擦力 (如床墊問題) 並不足以造成壓瘡,通常還要加上病人本身的因素 (如老人行動不便無法變更姿勢) 才會促成壓瘡。
肆、臨床表癥與分級
壓瘡最常發生於骶骨 (sacrum),其次為後腳跟 (calcaneus)、股骨大粗隆 (greater trochanter of femur) 等受壓迫的部位。而壓瘡的分級主要以傷口深度來分,可分成四期 (圖一)5。第一期為下壓不會反白的發紅區塊,若發生在皮膚黝黑的病人容易被忽略。第二期是指在表皮或真皮層的破損,通常沒有腐肉出現。第三期已達皮下脂肪層,可能有腐肉出現,但肌肉、韌帶或骨頭尚未暴露。第四期通常有腐肉出現,可能深及見骨,合併有坑道或隧道式傷口。但有些傷口基部被腐肉或焦痂遮蔽則無法確認深度與分級。
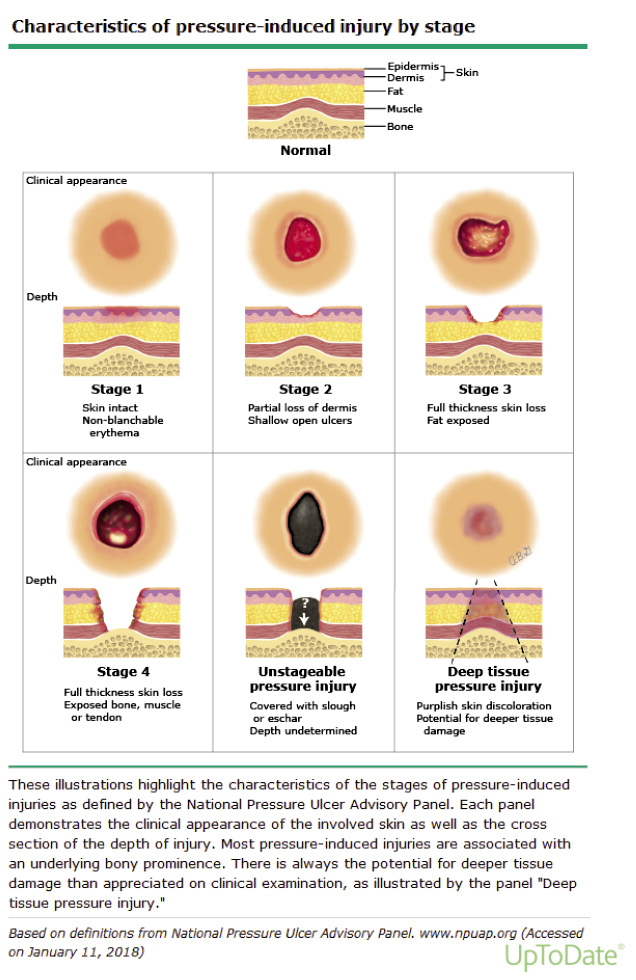
圖一 壓瘡分期5
伍、現行壓瘡的治療
一個有效的壓瘡治療計畫應包含營養支持、組織負荷管理與壓瘡傷口照護6。因為要有原料才可以長成新的組織,所以營養必須充足。組織負荷管理則經由減壓或改變姿勢,來降低促成壓瘡的壓力、剪力與摩擦力。壓瘡傷口照護則依據傷口程度決定進行局部清潔或清創;通常第三、四級的壓瘡才會考慮清創。傷口清潔須以乾淨取代無菌原則,以免消毒劑如碘酒會阻礙肉芽組織再生,可用生理食鹽水來清潔傷口。敷料選擇也是重點:傷口太乾會使角質細胞、纖維原細胞或其他生長因子無法覆蓋於傷口上而影響癒合;傷口太濕會使傷口腐爛惡化。對於局部傷口感染,可使用抗生素藥膏或口服抗生素;但若蜂窩性組織炎惡化或進展發生骨髓炎、敗血症則須輸注全身性抗生素7。
陸、現行壓瘡照護的困難
壓瘡屬於慢性傷口,有許多難以癒合的原因。病人如脊髓損傷者無法脫離長期坐臥狀態;肥胖病人脂肪較多導致血液供應較少,且翻身時易被拖拉;糖尿病病人因為組織糖分高,所以傷口特別難癒合;無法進食或食慾不佳的病人則易有營養不足的問題。另外,即使每兩小時幫病人翻身一次,還是可能因身體僵硬又翻回來壓到同處。
柒、Phenytoin 用於壓瘡的角色
Phenytoin 是一抗癲癇老藥,病人服用後其齒齦增生的發生率可達30-50%8。在1939年牙醫研究者即因此副作用發想 phenytoin 有促進傷口癒合之潛能1,之後陸續有不少臨床試驗往此方向進行。
Phenytoin 用於傷口癒合之機轉類似齒齦增生,可增加膠原蛋白的量促進傷口縮合與誘導生長因子促進血管新生。外敷 phenytoin 除了改變傷口 PH 值來降低細菌量外,亦能減少滲出液的產生9。一般用法為將一顆100 mg phenytoin 膠囊以5-20 mL 0.9% NaCl 稀釋,再拿紗布浸泡敷到傷口上,每日換藥。但用傳統敷料治療第二期壓瘡也有效,故外敷 phenytoin 用於第三期或第四期壓瘡會較有治療角色存在。
捌、 Phenytoin 用於壓瘡的相關臨床研究
2001年 Rhodes 等人將47位有第二級壓瘡的護理之家住民隨機分派至三組:DuoDerm 親水性膠體敷料、塗抹三合一抗生素藥膏與外敷 phenytoin (將一顆100 mg phenytoin 膠囊打開與5 mL 生理食鹽水混合,濃度為20 mg/mL)10。研究結果顯示,外敷 phenytoin 組在生成健康肉芽組織達傷口完全癒合的平均天數上,較其他兩組快 (phenytoin 組為35.3天,DuoDerm 敷料組為51.8天,三合一抗生素藥膏組為53.8天,p ≦ 0.05)。2007年 Subbanna 等人將28位因脊髓損傷臥床產生第二級壓瘡的住院病人隨機分派至兩組:外敷 phenytoin (將50 mg/mL 針劑用生理食鹽水稀釋到5 mg/mL) 與使用生理食鹽水11。研究結果顯示,外敷 phenytoin 組在壓瘡癒合評估量表 (PUSH,Pressure Ulcer Scale for Healing) 的降低分數,以及壓瘡大小減少的程度,都比生理食鹽水組高,但未達統計學上的顯著差異 (p = 0.261、p = 0.132);而在壓瘡體積減少的程度上,生理食鹽水組是較外敷 phenytoin 組多的,但也未達統計學上的顯著差異 (p = 0.777)。2008年 SN Sinha 等人報告非第二級以下壓瘡病人外敷 phenytoin 的案例12;其中一名52歲男性在左臀有第四級壓瘡,使用藻酸鹽敷料 (alginate rope) 三週後再加400 mg phenytoin 外敷,六週後左臀壓瘡明顯變淺與變小,此時再改為單用藻酸鹽敷料,其左臀壓瘡於第十四週完全癒合。
在國內的使用經驗上,台南市郭綜合醫院已有成功案例報告;其中有一名84歲男性患有高血壓與中風且長期臥床,下背部與小腿有嚴重壓瘡已至第四期。原本預計見骨的小腿必須截肢才能避免併發敗血症,但家屬不接受。由於經過兩個月的傳統療法如敷料與清創仍舊無法改善傷口,醫療團隊決定改用 phenytoin 100 mg 每天一次敷在傷口上,兩個月後這兩處壓瘡已長出新肉 (圖二、三)。
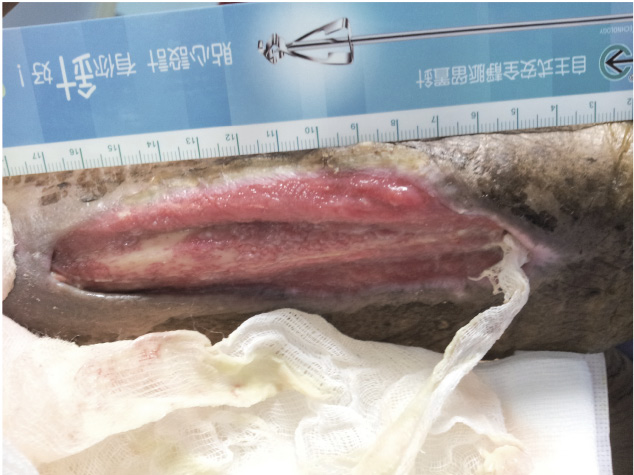
圖二 未外敷 phenytoin 前之壓瘡,於小腿處已見骨
圖三 外敷 phenytoin 兩個月後小腿處壓瘡生成新肉,已無見骨
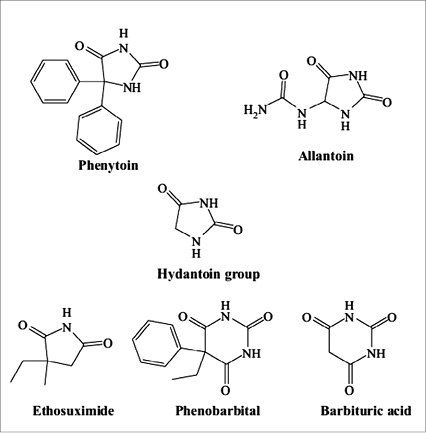
另外,有研究推論 phenytoin 的藥化結構含 hydantoin group (圖四) 可能與傷口修復有關,故有研究探討是否其他與 phenytoin 藥化結構類似的抗癲癇藥也有促進傷口癒合之潛能?結果發現使用 ethosuximide 與 phenobarbital 的病人都有傷口癒合之趨勢13。

圖四 phenytoin、allantion、ethosuximide 與 barbituric acid 的藥化結構中都有 hydantoin group14
玖、外敷 phenytoin 的注意事項
外敷 phenytoin 的副作用多為刺痛與灼熱感,但若傷口太深其皮膚的痛覺受器已遭破壞,這類副作用是可忽略的。目前對於局部使用 phenytoin 治療壓瘡的最佳藥物劑型與劑量並無定論,但考量用膠囊或針劑去稀釋,其低溶解度與高 PH 值可能會傷害組織細胞,故有國家如中東發展出專門外用的製劑 (Healosol spray:phenytoin 2%,此製劑亦可用於糖尿病足與燒傷等傷口)。
外敷 phenytoin 其全身性吸收是非常少的,大多臨床試驗都測不到血中濃度;有一位需要每日使用12.5 g phenytoin 覆蓋大型壓瘡的病人,一個月後測 phenytoin 血清濃度為4.3 mg/L,遠低於其安全監測範圍10-20 mg/L14。另外,傷口達癒合的療程多為2-3個月,所以口服 phenytoin 常見的副作用幾乎不會發生。
拾、結論
雖然外敷 phenytoin 治療壓瘡已有研究證實有療效,護理端執行起來不難且花費低,目前在台灣這樣的用法仍是仿單標示外使用 (off-label use)。最近,雖然在2017年有一篇系統性回顧文章提到外敷 phenytoin 用於第一期或第二期壓瘡的療效是否優於傳統敷料仍不明確,但本文收錄的研究證據等級偏低15。因此,關於外敷 phenytoin 治療壓瘡的最佳劑量與劑型,仍需要更多大規模的臨床試驗來作確認。
Topical Phenytoin for Treating Pressure Ulcers
Yi-Nong Lin1, Chia-Ling Chen2, Yu-Lin Yang3
Department of Pharmacy, Tainan Municipal Hospital1
Department of Pharmacy, Kuo General Hospital2
Department of Home Care Nursing, Kuo General Hospital3
Abstract
Pressure ulcers (PUs) are lesions caused by unrelieved pressure that results in damage to the underlying tissue. Apart from causing suffering to patients, PUs also result in increased length of hospital stay and cost of health care. Modern available dressings such as hydrocolloids work well in Stage I and II PUs.
Phenytoin is an anticonvulsant drug and gingival hyperplasia is recognized as its adverse effect, which suggested possible use as a healing agent in wounds. Phenytoin may be involved in several healing process such as promoting deposition of collagen and other connective tissue, decreasing bacterial contamination and reducing wound exudate production. Topical phenytoin play a significant role in Stage III and IV PUs. The side effects of oral phenytoin have not been reported in the topical phenytoin for wound healing because of the minimal systemic absorption. The formulation of phenytoin solution from pills, capsules or intravenous use is inconvenient for topical use because of low solubility and high pH, which may have stinging and burning sensations. In PU the pain is absent or reduced due to destruction of sensory receptors. Further clinical trials are recommended to evaluate the optimal topical dose and the use of a delivery vehicle.
參考資料:
1.Kimball OP, Horan TN. The use of Dilantin in the treatment of epilepsy. Ann Intern Med. 1939;13:787-93.
2. Shapiro M. Acceleration of gingival wound healing in non-epileptic patients receiving diphenylhydantoin sodium. Exp Med Surg. 1958;16:41-53.
3. Lyder CH, Wang Y, Metersky M, et al: Hospital-acquired pressure ulcers: results from the national Medicare Patient Safety Monitoring System study. J Am Geriatr Soc. 2012;60(9):1603-8.
4. Brandeis GH, Morris JN, Nash DJ, et al: The epidemiology and natural history of pressure ulcers in elderly nursing home residents.
JAMA. 1990;264(22):2905-9.
5. National Pressure Ulcer Advisory Panel. [homepage on the Internet]. Washington: The Association; 2018[cited 2018 Apr 2]. Available from: http://www.npuap.org/.
6. European pressure ulcer Advisory Panel. [homepage on the Internet]. Prague: The Association; 2014[cited 2018 Apr 2]. Available from: http:// www.epuap.org/.
7. Lipsky BA, Hoey C. Topical antimicrobial therapy for treating chronic wounds. Clin Infect Dis. 2009;49(10):1541-9.
8. T. Modéer, H. Domeij, I. Andurén, et al: Effect of phenytoin on the production of interleukin-6 and interleukin-8 in human gingival fibroblasts. Journal of Oral Pathology and Medicine. 2000;29(10):491-9.
9. Ashima Bhatia MD, Surya Prakash DVD. Topical phenytoin for wound healing. Dermatology Online Journal. 2004;10(1):5.
10. Richard S Rhodes, Catherine A Heyneman, Vaughn L Culbertson, et al: Topical Phenytoin Treatment of Stage II Decubitus Ulcers in the Elderly. The Annals of Pharmacotherapy. 2001;35(6):675-81.
11. PK Subbanna, FX Margaret Shanti1, J George, et al: Topical phenytoin solution for treating pressure ulcers a prospective, randomized, double-blind clinical trial. Spinal Cord. 2007;45:739-43.
12. Sinha SN, Amarasena I. Does phenytoin have a role in the treatment of pressure ulcers? Wound Practice and Research. 2008;16:37-41.
13. Dema M. Ajwee, Ahmad M. Disi, Eyad A. Qunaibi, et al: Ethosuximide and Phenobarbital Promote Wound Healing via Enhancing Collagenization. Chem Biol Drug Des. 2012;79:137-42.
14. Anstead GM, Hart LM, Sunahara JF & Liter ME. Phenytoin in wound healing. Ann Pharmacol 1996; 30:768-75.
15. Hao XY, Li HL, Su H, et al.Topical phenytoin for treating pressure ulcers. Cochrane Database Syst Rev. 2017;22:2 CD008251.
通訊作者:陳佳玲/通訊地址:台南市中西區民生路二段22號
服務單位:郭綜合醫院藥劑科藥師/聯絡電話:(O) 06-2221111 ext 2155

