摘要
高血壓是引起粥狀動脈硬化心血管疾病 (ASCVD;atherosclerotic cardiovascular disease)、心衰竭、微血管併發症等疾病的強烈危險因子,很多研究顯示高血壓的控制與治療,可預防或延緩糖尿病人 ASCVD 的進行,減少大小血管併發症的發生。隨機臨床試驗與統合分析的實證支持,大部分成年糖尿病人之血壓控制目標值至少要小於140/90 mmHg,然而對於高心血管疾病風險之糖尿病人,較低的血壓控制目標 (小於130/80 mmHg) 相對是有益的。除了生活型態的調適外,為了達成血壓控制目標,通常需要合併多種類藥物來治療。ACEI (angiotensin converting enzyme inhibitor)、ARB (angiotensin receptor blocker)、dihydropyridine CCB (calcium channel blocker)、thiazide-like diuretic 可改善臨床結果,是血壓控制的較優選項,而對於有蛋白尿的病人 ACEI 或 ARB 是首選。高血壓的治療將基於病人的共病症,預期減少大小血管併發症的好處,發生不良事件的風險等個別化因素來考量。
關鍵字:高血壓、ASCVD、糖尿病、ACEI、ARB
壹、前言
粥狀動脈硬化心血管疾病 (ASCVD;atherosclerotic cardiovascular disease) 包含冠心病、腦血管疾病、周邊動脈疾病和心衰竭等,它是導致糖尿病人住院與死亡的最主要原因。然而高血壓是引發 ASCVD、心衰竭、微血管併發症等疾病的強烈危險因子,很多研究證實,高血壓的控制與治療可預防或延緩 ASCVD 的進行,減少大小血管併發症的發生1-4。以下文章內容針對血壓的處理與治療等相關議題來討論。
貳、高血壓與血壓之控制
高血壓的一般定義是血壓持續 ≥ 140/90 mmHg,它是引起 ASCVD 和微血管併發症的主要危險因子,研究證實治療高血壓可減少 ASCVD、心衰竭和微血管併發症的風險1-4。
一、治療目標
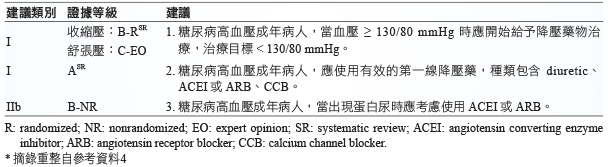
隨機臨床試驗顯示血壓控制 < 140/90 mmHg 可減少心血管事件和微血管併發症的發生5-6。因此一般高血壓糖尿病人之血壓治療目標最少要 < 140/90 mmHg;然而對於高心血管疾病風險之糖尿病人,應加強血壓控制,治療目標 < 130/80 mmHg1,2,4,(表一)4、(圖一)1,2。
表一 糖尿病人高血壓之治療建議*
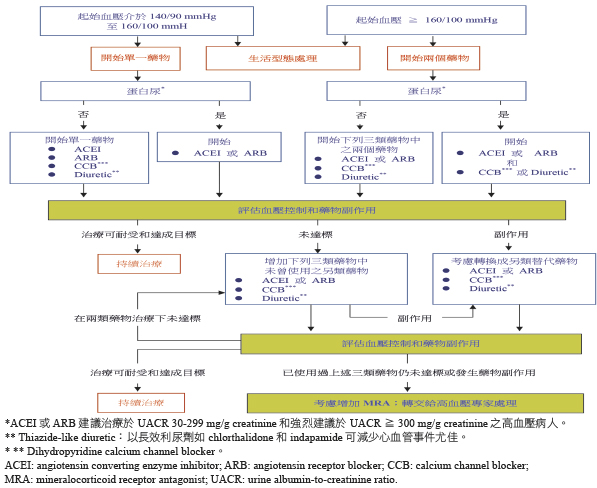
圖一 糖尿病高血壓病人之治療推薦流程1-2
(一) 隨機臨床試驗之血壓控制 (加強治療 vs 標準治療)
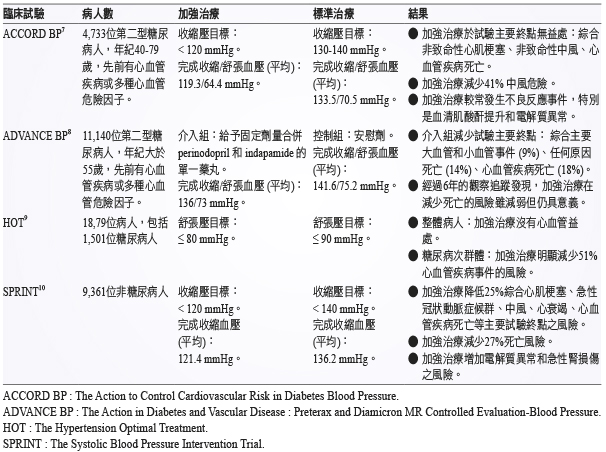
在 ACCORD BP (The Action to Control Cardiovascular Risk in Diabetes Blood Pressure) 的研究顯示7,加強血壓控制 (收縮壓目標 < 120 mmHg) 對比標準血壓控制 (收縮壓目標 < 140 mmHg),並未減少總 ASCVD 事件,但可減少中風的風險。其它相關研究試驗的結果7-10,(表二)1,2。
表二 隨機控制試驗之高血壓治療對策 (加強治療 vs 標準治療)1-2
(二)統合分析試驗
基於統合分析試驗顯示,當糖尿病人平均基礎血壓 ≥ 140/90 mmHg 或平均達標血壓 (加強治療) ≥ 130/80 mmHg 時,給予降壓治療是有益處的。然而在基礎血壓或達標血壓較低的情況下,降壓治療仍可減少中風、視網膜病變和蛋白尿的風險,但在減少其它 ASCVD 和心衰竭的結果並未有明顯的意義2,5,6。
(三)治療目標個別化
影響血壓治療目標的因素包含治療的風險 (如低血壓、藥物不良反應)、預期壽命、共病症、病人態度、外來資源等11。當糖尿病人有較高心血管事件風險或蛋白尿,同時執行加強血壓控制相對較容易時,則適合給予加強血壓控制目標的治療;相反的,老年人常見身體功能受限、服用多種藥物、合併多種併發症,較適合給予非加強血壓控制目標的治療1。
二、治療策略
(一)生活型態治療
生活型態的調適是高血壓治療的一項重要方式,它可以降低血壓、加強某些降壓藥療效、促進代謝和較少不良反應發生。生活型態的治療包含限制卡路里和鈉鹽 (< 2300 mg/day) 的攝取、增加蔬果和低脂乳製品耗用、避免過量飲酒、增加活動量等方式而達到減重降壓效果。
當糖尿病人血壓微上升 (收縮壓 > 120 mmHg 或舒張壓 > 80 mmHg) 應給予上述的生活型態治療;而當高血壓被診斷時,除了合併生活型態介入外應開始給予降壓藥物治療1-2。
(二)藥物治療
1.降壓藥的起始數:
糖尿病人血壓之起始治療可依據高血壓的嚴重度做選擇 (圖一)1-2,當血壓介於140/90至160/100 mmHg 之間,可開始給予單一藥物治療;若血壓 ≥ 160/100 mmHg,為了更有效的控制血壓則建議給予兩種降壓藥當作起始治療。
2.降壓藥的分類:
降壓藥的起始治療將包含可以減少糖尿病人心血管事件之藥物種類如 ACEI (angiotensin converting enzyme inhibitor)、ARB (angiotensin receptor blocker)、thiazide-like diuretic 或 dihydropyridine CCB (calcium channel blocker)1-4,(表一)4、(圖一)1-2。糖尿病蛋白尿病人當 UACR (urine albumin-to-creatinine ratio) ≥ 30 mg/g,為了減少腎疾病惡化的風險則起始治療應包含 ACEI 或 ARB (表一)4、(圖一)1-2。
3. 多種類藥物治療:
要達成血壓控制目標通常需要合併多種類藥物一起治療,特別是在糖尿病腎疾病的情況下。然而 ACEI 與 ARB 的合併治療並不被 ADA (American Diabetes Association) 推薦12,因為合併此兩類藥物治療缺乏減少 ASCVD 的好處,同時可能增加高血鉀、昏厥和急性腎損傷等不良反應事件的風險。
4.糖尿病腎疾病:
糖尿病合併蛋白尿病人當 UACR ≥ 30 mg/g creatinine,特別是 ≥ 300 mg/g creatinine時,會增加腎疾病惡化的風險。而 ACEI 和 ARB 有獨特的腎保護作用,可延緩腎疾病惡化,在此種情況下為降壓藥首選1-4。
5. 高血鉀和急性腎損傷:
ACEI 或 ARB 個別藥物可能引起高血鉀和急性腎損傷;利尿劑則依據不同的作用機轉,可能引起急性腎損傷和高血鉀或低血鉀。由於急性腎損傷和高血鉀會增加心血管事件和死亡風險,監測與處理這些異常情況顯得非常重要,因此當給予 ACEI、ARB 或利尿劑治療時,應監測血清肌酸酐和鉀離子值,特別是腎絲球過濾率已減少的病人13。
(三)頑固性高血壓
頑固性高血壓的定義是雖然給予適當的生活型態處理,並加上利尿劑和兩種不同類降壓藥足夠劑量治療下,血壓仍 ≥ 140/90 mmHg。研究顯示第二型糖尿病人在 ACEI 或 ARB、thiazide-like diuretic 和 dihydropyridine CCB 等降壓藥治療下,增加 MRA (mineralocorticoid receptor antagonist) 可有效治療頑固性高血壓,同時也可減少蛋白尿和心血管風險14。然而當 MRA 與 ACEI 或 ARB 併用時可能增加高血鉀風險,因此常規監測血清肌酸酐和鉀離子值益顯重要。
(四)懷孕與降壓藥
由於缺乏隨機控制試驗於糖尿病懷孕婦女之降壓治療分析,因此其治療推薦類似於所有懷孕婦女。且由於無法確認治療的好處優於潛在的風險,ACOG (The American College of Obstetricians and Gynecologists) 建議低中度妊娠高血壓 (收縮壓 < 160 mmHg 或舒張壓 < 110 mmHg) 病人,不需要給予降壓藥治療15。然而對於有心血管或腎疾病等標的器官受損的懷孕婦女,可考慮降低血壓控制目標以避免懷孕期間這些標的器官受損的情況惡化。由於 ACEI、ARB 或 spironolactone 可能致畸胎,因此禁用於懷孕婦女。對於懷孕婦女有效且安全的降壓藥包括 methyldopa、labetalol 和 long-acting nifedipine,而 hydralazine 可考慮用於懷孕高血壓或嚴重子癇前症的緊急處理15。
參、結論
高血壓是引發糖尿病大小血管併發症的強烈可修正危險因子,文獻資料顯示多種降壓藥在預防大小血管併發症的臨床療效。隨機臨床試驗與統合分析的實證支持大部分成年糖尿病人之血壓控制目標值至少要小於140/90 mmHg,然而對於高心血管疾病風險之糖尿病人,較低的血壓控制目標 (小於130/80 mmHg) 相對是有益的,目標值可依據個別病人之基本狀況來衡量。除了生活型態的調適外,為了達成血壓控制目標,通常需要合併多種類藥物來治療。ACEI、ARB、dihydropyridine CCB、thiazide-like diuretic 可改善臨床結果,是血壓控制的較優選項,而對於有蛋白尿的病人 ACEI 或 ARB 是首選。高血壓的治療藥物選擇將基於病人的共病症,預期減少大小血管併發症的好處,發生不良事件的風險等個別化因素來考量。
Standards of Medical Care in Diabetes: Hypertension Management and Treatment
Chun-Chi Chiou, Ching-Ling Tai
Department of Pharmacy, Kaohsiung Chang Gung Memorial Hospital
Abstract
Hypertension is a strong risk factor for atherosclerotic cardiovascular disease (ASCVD), heart failure, and microvascular complications. Numerous studies have shown that the control and therapy of hypertension in preventing or slowing ASCVD, reducing the macrovascular and microvascular complications in people with diabetes. Strong evidence from randomized clinical trials and meta-analyses supports targeting blood pressure reduction to at least < 140/90 mmHg in most adults with diabetes. Lower blood pressure targets (< 130/80 mmHg) may be beneficial for high cardiovascular disease risk. In addition to lifestyle modifications, multiple medication classes are often needed to attain blood pressure goals. ACEI (angiotensin converting enzyme inhibitor), ARB (angiotensin receptor blocker), dihydropyridine CCB (calcium channel blocker), thiazide-like diuretic have been demonstrated to improve clinical outcomes and are preferred for blood pressure control. For patients with albuminuria, ACEI or ARB should be first choice. Hypertension treatment should be individualized based on their comorbidities, their anticipated benefit for reduced the macrovascular and microvascular complications, and their risk of adverse events.
參考資料:
1. American Diabetes Association. 9. Cardiovascular disease and risk management: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018;41(Suppl. 1):S86-S104.
2. de Boer IH, Bangalore S, Benetos A, et al: Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes Care 2017;40:1273-1284.
3. Low Wang CC, Hess CN, Hiatt WR et al: Clinical update: cardiovascular disease in diabetes mellitus: atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus – mechanisms, management, and clinical considerations. Circulation 2016; 133: 2459–2502.
4. Whelton PK, Carey RM, Aronow WS, et al: 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018;71:e13-e115.
5. Emdin CA, Rahimi K, Neal B, Callender T, Perkovic V, Patel A. Blood pressure lowering in type 2 diabetes: a systematic review and meta-analysis. JAMA 2015;313:603-615.
6. Ettehad D, Emdin CA, Kiran A, et al: Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 2016;387:957-967.
7. Cushman WC, Evans GW, Byington RP, et al: ACCORD Study Group. Effects of intensive bloodpressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-1585.
8. Patel A, MacMahon S, Chalmers J, et al: ADVANCE Collaborative Group. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet 2007; 370:829-840.
9. Hansson L, Zanchetti A, Carruthers SG, et al: HOT Study Group. Effects of intensive bloodpressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet 1998;351:1755-1762.
10. Wright JT Jr, Williamson JD, Whelton PK, et al: SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015;373:2103-2116.
11. Association AD; American Diabetes Association. Glycemic targets. Sec. 6. In Standards of Medical Care in Diabetes-2017. Diabetes Care 2017;40(Suppl. 1):S48-S56.
12. American Diabetes Association. 8. Cardiovascular disease and risk management. Diabetes Care.2016;39 (Suppl. 1):S60-S71.
13. James MT, Grams ME, Woodward M, et al: CKD Prognosis Consortium. A meta-analysis of the association of estimated GFR, albuminuria, diabetes mellitus, and hypertension with acute kidney injury. Am J Kidney Dis 2015;66:602-612.
14. Williams B, MacDonald TM, Morant S, et al: British Hypertension Society's PATHWAY Studies Group. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet 2015;386:2059-2068.
15. American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists' Task Force on Hypertension in Pregnancy. Obstet Gynecol 2013;122:1122-1131.
通訊作者:邱春吉/通訊地址:高雄市鳥松區大埤路123號
服務單位:高雄長庚紀念醫院藥劑部藥師/聯絡電話:(O) 07-7317123 ext 6274

