Escitalopram治療重度憂鬱症之探討
歐佳傑1,2、林湛學1,2、李威德1,2、朱育瑩1,2、謝永宏1,3
1光田綜合醫院藥劑部、2台中市新藥師公會、3弘光科技大學
摘要
選擇性血清素回收抑制劑(selective serotonin reuptake inhibitors, SSRIs)已漸漸成為主要治療重度憂鬱症(major depressive disorder, MDD)的藥物。SSRIs的療效整體上差異不大,但在藥物特性、產生療效的快慢則有明顯的差異,治療初期常見的難題在於副作用比療效更早出現,患者會認為藥物無效且症狀加劇而自行停藥,造成發生停藥症候群的風險。
因escitalopram除了作用於血清素轉運體(serotonin transporter, SERT)的正構位(primary site)外,還作用於異構位(allosteric site),促進escitalopram在正構位的結合,加強提高血清素(serotonin, 5-HT)濃度的效果,增加緩解率。escitalopram較高的專一性也使副作用發生減少且症狀輕微,合理作為MDD病人在SSRIs中的優先選擇。另外文獻發現,escitalopram使用10mg以上的劑量,其escitalopram血清濃度(serum concentration of escitalopram, SCE)到達治療閾值後(20ng/mL)和抗憂鬱反應(antidepressant response, AR)之間沒有顯著正相關,但目前還需要更多試驗和文獻證明這項關聯性,以進一步了解高劑量escitalopram在MDD病人身上的治療效果。
關鍵字: 重度憂鬱症、抗憂鬱反應、SSRIs、MDD、escitalopram、antidepressant response
壹、 前言
現代社會對心理健康的關注不亞於對身體健康的重視,影響心理層面最廣為所知的便是憂鬱症。典型憂鬱症會出現情緒低落,對許多事物不感興趣,自尊心下降及無精神等消極狀態1,甚至有生理上的症狀,包含不明疼痛、妄想或幻覺1,是使人身心極度衰弱的疾病,對於個人及社會都傷害甚大,不可不重視。
2015年全世界約2.16%的人患有憂鬱症2,已開發國家終身盛行率達15%3,憂鬱症導致的死亡雖不比其它疾病,但現今人們追求活得有品質,在反映疾病對生活品質影響的數據「健康生命損失年」中,憂鬱症排名第二,僅次於下背部疼痛2。
憂鬱症細分多種,依程度和持續時間大致分為輕度、重度及季節性憂鬱4,輕度憂鬱症現稱持續型憂鬱症,輕微但持續久,至少兩年(青少年為一年),多數時間處於憂鬱狀態;重度憂鬱症是症狀嚴重影響生活,持續兩週以上;季節性憂鬱症症狀不若MDD嚴重,好發於日照少的季節。
憂鬱症成因包含遺傳、環境、心理等,遺傳約占四成5。治療手段包含心理諮商、藥物治療及電痙攣治療,一般以心理諮商優先,但情況較嚴重,如MDD病人一個月內自殺率可達3%6,就會配合藥物或電痙攣治療。本文將著重藥物治療,探討選擇性血清素回收抑制劑在MDD病人的使用,針對SSRIs中的escitalopram與其它SSRIs藥物進行比較與深入探討。
貳、SSRIs藥物簡介
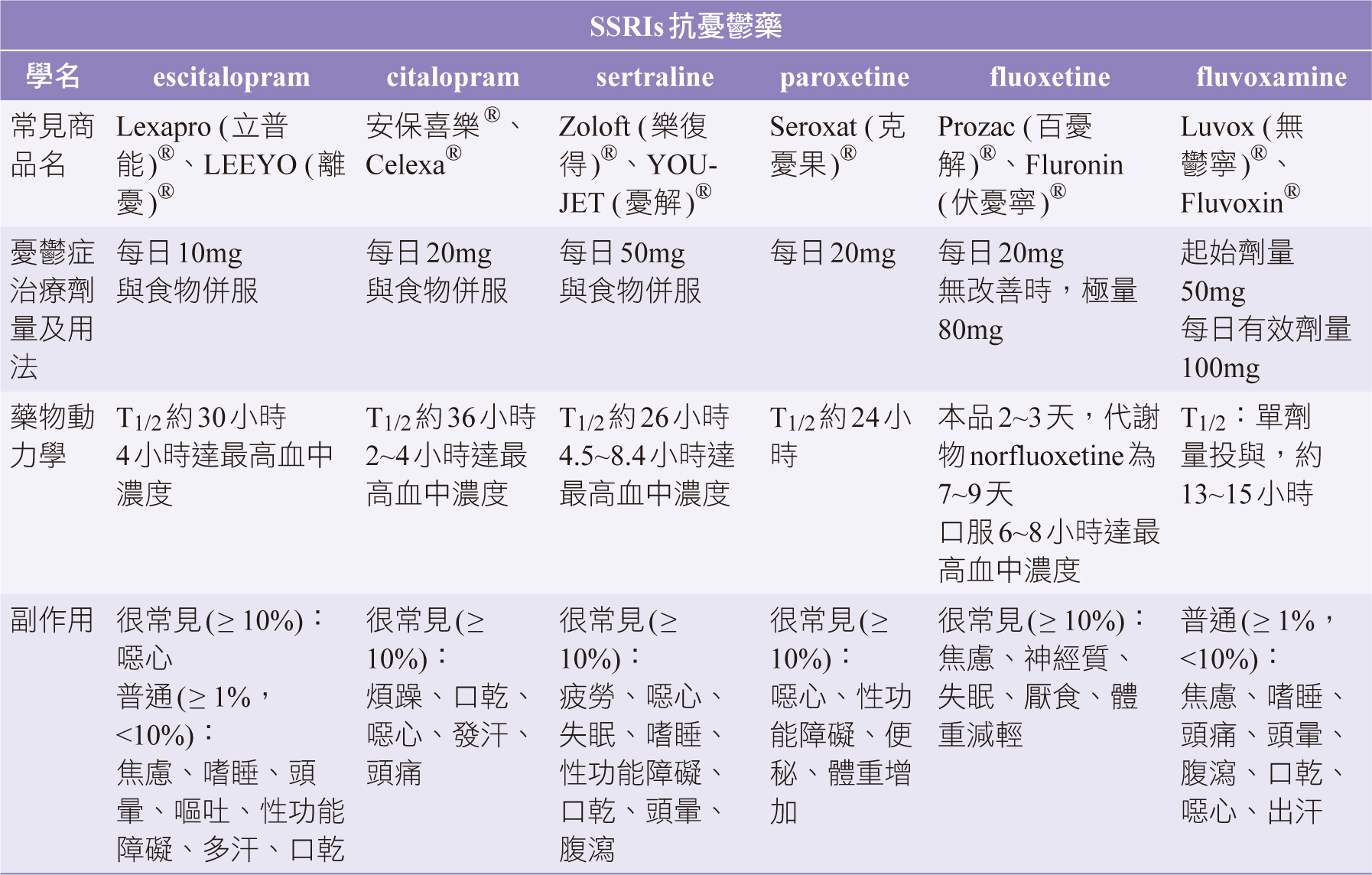
SSRIs療效整體差異不大,不同在於藥物特性和常見副作用,選擇藥品時,須考量個案狀況,包含用藥時避免交互作用或個案是否能忍受副作用。SSRIs副作用常較療效先出現,常見副作用包括焦躁不安、腸胃不適,通常在服藥第二週時逐漸減輕,多數SSRIs藥效需二到四週才明顯發揮。治療初期副作用與原本焦慮憂鬱症狀相似,常使患者認為藥物無效且加重症狀,導致中斷療程,錯過黃金治療期,是治療一大難題4。SSRIs藥物劑量的調整,須視治療效果和能否忍受副作用而定。針對目前市面上治療MDD的主流SSRIs品項資訊整理如表一7。
參、 文獻探討
一、SSRIs藥物對MDD病人療效和安全性比較
關於SSRIs藥物間的療效評估常用以下兩種評估表,其一是蒙哥馬利-阿斯伯格憂鬱評估量表(Montgomery-Asberg Depression Rating Scale, MADRS),其二是漢彌爾頓憂鬱評估量表(Hamilton Rating Scale for Depression, HRS-D),此外治療期間的不良事件(treatment emergent adverse event, TEAE)用於評估安全性與副作用。
Vaya Lalit等人進行多中心隨機雙盲試驗8,總共214位MDD且HRS-D>18分的病人,74位給予escitalopram、69位給予citalopram、71位給予sertraline,4週後評估療效發現,escitalopram相對於citalopram有較高的反應率(症狀減輕,定義為HRS-D評分<基線50%)與緩解率(症狀幾乎消失或完全消失,定義為HRS-D評分<8分),反應率分別為90%與86%、緩解率為74%和65%,此外發現sertraline在最初2週的療效不如escitalopram,但治療4週後反應率為97%,優於escitalopram的90%,說明sertraline於MDD急性期療效可能弱於escitalopram,但與MDD短期療效比較時,escitalopram的反應率不劣於sertraline。
為擴大研究escitalopram與其它SSRIs使用於MDD的療效和中斷療程機率,AG Wade等人進行為期6個月之隨機、雙盲試驗9,共納入1398位MDD病人,一組給予escitalopram 10mg、另一組作為對照組隨機給予citalopram、duloxetine、paroxetine藥物,研究顯示escitalopram對MDD病人的緩解率(MADRS≤10)為70.7%、完全緩解率(MADRS≤5)為51.7%,皆顯著高於對照組(p<0.01),且使用escitalopram的病人中斷療程的比率比隨機給予citalopram、duloxetine、paroxetine之對照組來的低,分別為15.9%與23.9%(p<0.001)。
Tianmei Si等人研究納入255位MADRS>30分的MDD病人10,給予escitalopram 進行為期8週的治療後,escitalopram緩解率為72.9%,p<0.0001(MADRS≤10分)。其中有28.38%的病人治療後出現TEAE,常見的TEAE有嗜睡(9.0%)、噁心(7.7%)、多汗症(4.5%)、口乾(4.1%)、頭暈(4.1%);其它SSRIs常見的副作用如焦慮、失眠、性功能障礙的發生則相對較少。
表一 主流SSRIs品項資訊7
二、SSRIs藥物耐受性比較
統合分析針對117項的隨機對照試驗11,納入25,928人的MDD病人,比較12項抗憂鬱藥物。在比較最佳治療方法中,escitalopram的可接受度最高(27.6%),也較少發生停藥症候群,接受度次高的sertraline(21.3%),其常見的副作用腹瀉發生率高於esitalopram(OR: 2.10, 【95%CI】:1.22~3.61, p=0.007)12,整體不良事件發生率亦高於esitalopram(OR: 1.76, 【95%CI】:1.06~2.94, p=0.03)。
可接受度低的paroxetine(0.2%)比其它SSRIs不良反應發生率更高11,包括噁心、便秘、性功能障礙以及體重增加,因為paroxetine毒蕈鹼受體親和力大,易引起許多副作用,導致病人耐受性差11,13,另外paroxetine也抑制CYP2D6,是較易引起藥物交互作用的SSRIs(表二)13。
表二 escitalopram、paroxetine和sertraline藥物交互作用和藥效學特性13

三、SSRIs藥物作用機轉
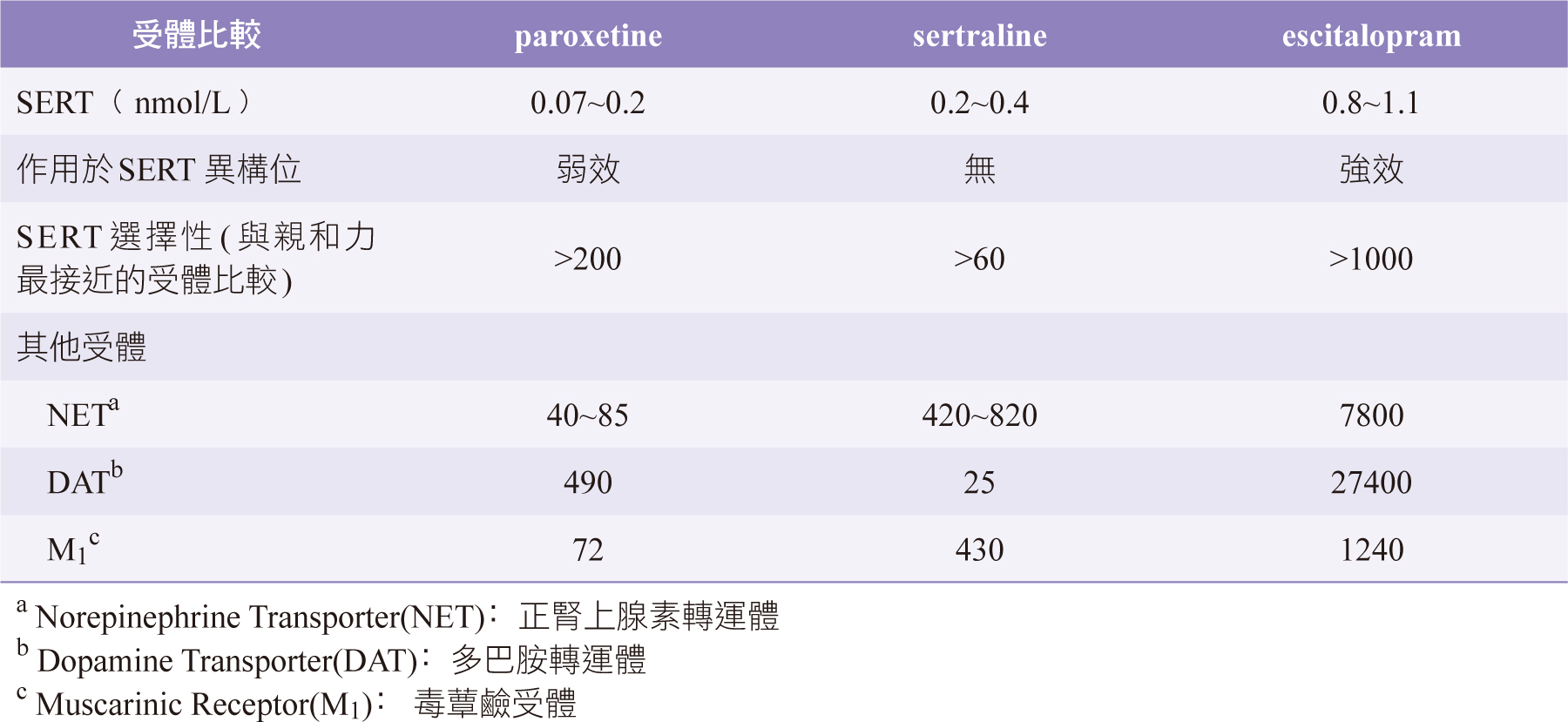
Escitalopram、sertraline和paroxetine在腦內血清素轉運體佔用率(serotonin transporter occupancy, SERT Occupancy)的增加和細胞外血清素(serotonin, 5-HT)的濃度升高有關13,要產生足夠抗鬱效果,須達近80%的SERT Occupancy、escitalopram約10天,而paroxetine和sertraline則需約4週(表二)13,因escitalopram選擇性最高(約>1000倍,代表escitalopram抑制其它受體所需的濃度至少大於抑制SERT所需濃度1000倍,paroxetine和sertraline分別為>200倍和>60倍),而paroxetine和sertraline對其它受體亦有高度親和力(表三)13,需花更多時間才能達到80%的SERT Occupancy。
相同SERT Occupancy下,不同SSRIs藥物提升5-HT濃度的效果有差異13。相同SERT Occupancy時,escitalopram比paroxetine和sertraline能產生更高的細胞外5-HT 濃度,原因除了其它SSRIs與SERT結合的正構位外13,14,escitalopram還結合在SERT異構位,加強escitalopram在正構位的結合,提升抑制效果。escitalopram進一步分類為異構位血清素回收抑制劑(allosteric serotonin reuptake inhibitor, ASRI)13,其它SSRIs如sertraline、fluoxetine,只能透過正構位的結合抑制SERT(圖一)13。
表三 escitalopram、paroxetine和sertraline於各項受體親和力強弱13
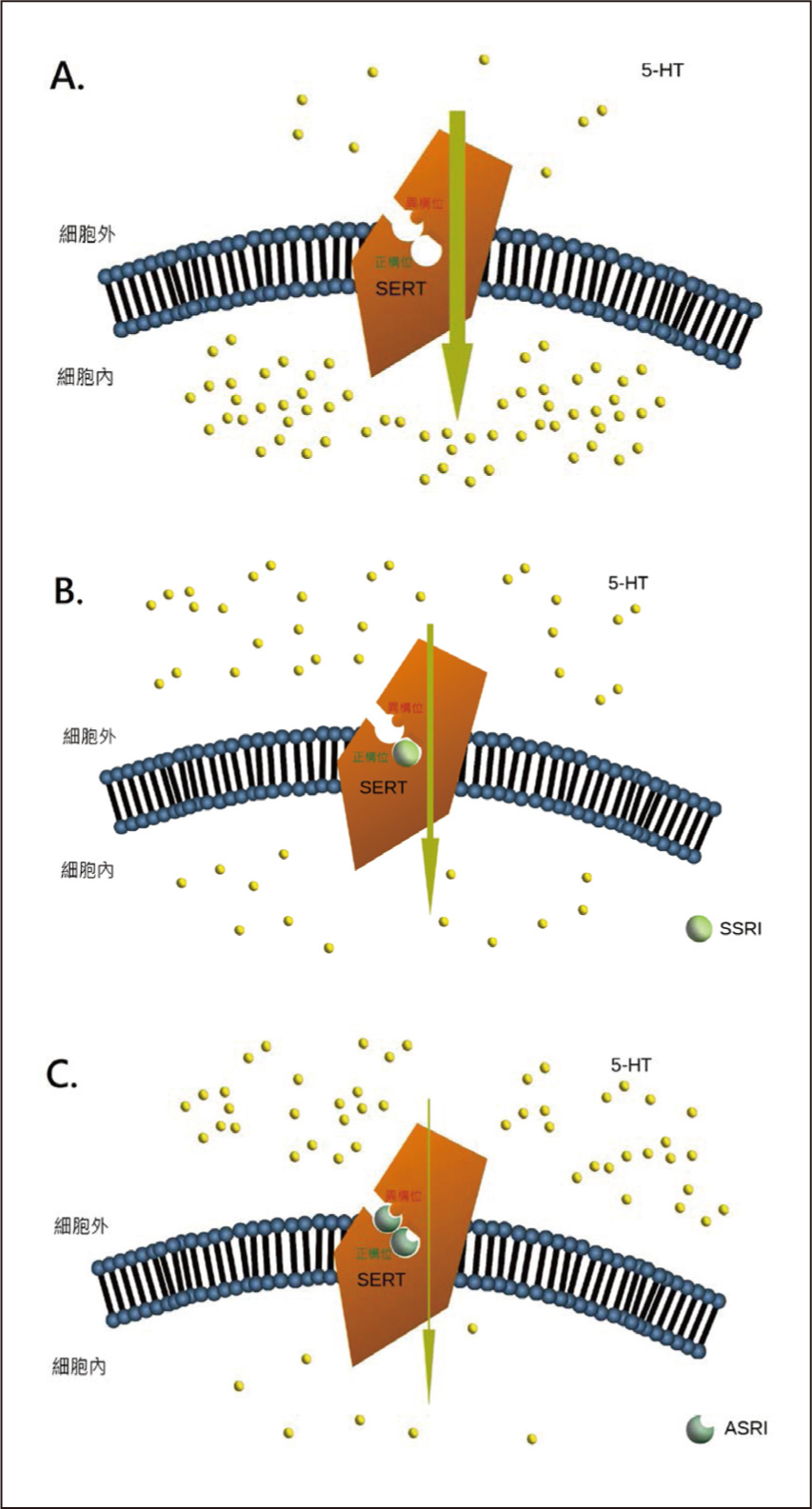
圖一 escitalopram(ASRI)和一般SSRIs結合在正構位或異構位時,呈現出神經細胞外的5-HT濃度高低差異13
A. 無SSRIs時,神經細胞外的5-HT濃度偏低。
B. 一般SSRIs僅結合在SERT正構位時,會促進神經細胞外的5-HT濃度提高。
C. 具ASRI特性的SSRIs(escitalopram)同時結合在SERT正構位和異構位時,更促進神經細胞外的5-HT濃度大幅提高。
基於SERT Occupancy要達到80%,Kasper認為血清濃度要高於20ng/mL(治療閾值)15,但escitalopram有異構位調節機制,大幅提高5-HT濃度14。要探討escitalopram血清濃度與抗憂鬱反應的關聯,Vincenzo F等人納入70位MDD病人(HRS-D17平均23.8)15,給予escitalopram治療(第1個月與第3個月)。整體顯示,HRS-D17第1月降至17.18(p<0.001),第3月再下降至13.73(p=0.0003),且SCE和AR存在正相關。但排除SCE<20ng/mL的患者,SCE和AR的關聯性不明顯,說明濃度在治療閾值之下時,SCE和AR呈直接正相關(病人的AR是較弱的),但超過閾值,SCE和AR卻沒有顯著的正相關(圖二)15。
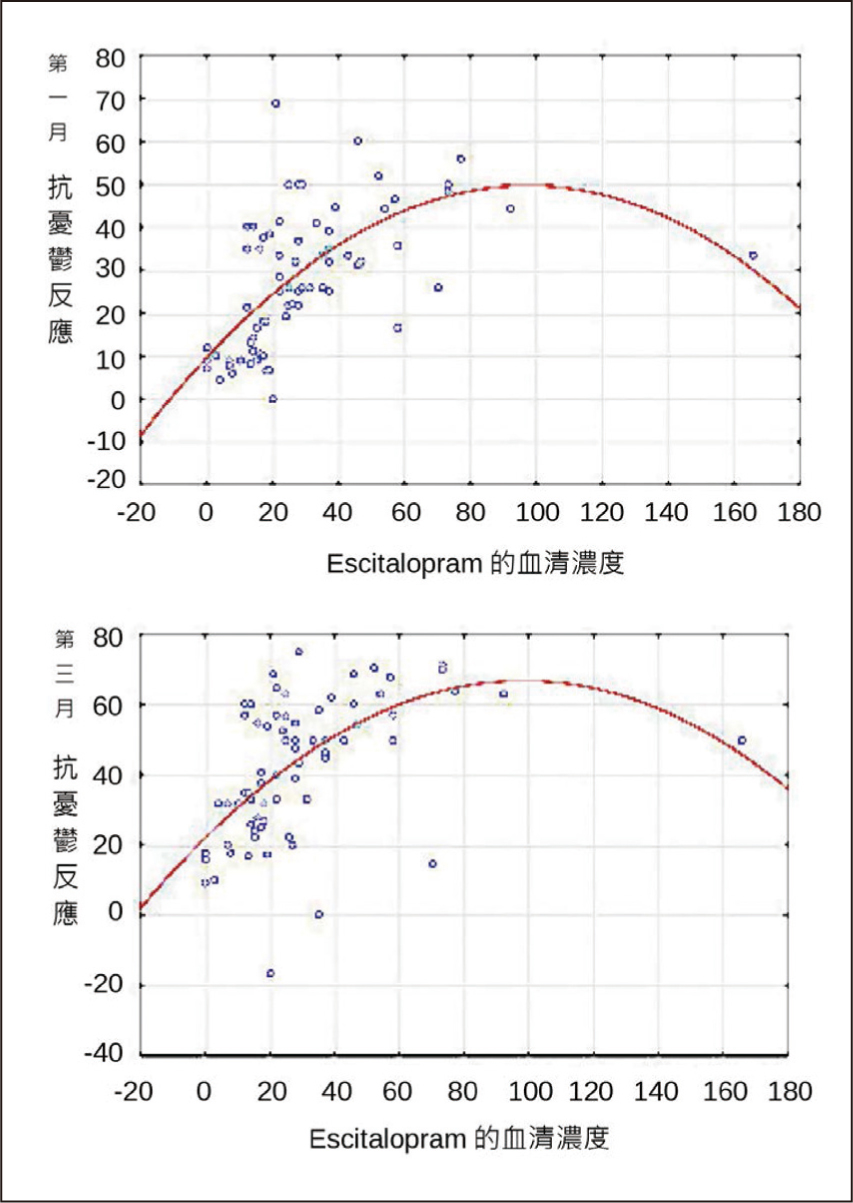
圖二 SCE和AR間的關聯性(第一月和第三月):SCE<20ng/mL(治療閾值) 時,呈現正相關,>20ng/mL時呈現較大變異數(關聯性不明顯)15
變異數(Variance):算出各個數據分布、零散(相對中心點)程度
肆、討論
文獻得知escitalopram因結構特性(ASRI),經專一性結合在SERT正構位和異構位13,14,引起更完全且持續的5-HT回收抑制功效,以較低劑量帶來比消旋體citalopram更好的療效與更少的副作用8,且相當於sertraline的藥物反應率和緩解率8。
Escitalopram從開始到產生足夠療效僅需10天,且達到血中最高濃度迅速(4小時)13,適合MDD的急性期和短期治療(8週)。Escitalopram的TEAE僅為輕微反應如噁心、嗜睡、多汗、疲倦等10,發生率1~10%,低於其他SSRIs7。雖然有口乾、焦慮等副作用,但發生率低,所以病人中斷療程比率低7,9,加上8週後的緩解率可能會增加,Wade推斷短期治療可預測長期治療的可接受度9。雖然sertraline有更高的SERT結合率和症狀緩解率8,13,但因為有較高的副作用機率(性功能障礙、腹瀉、失眠、頭痛等TEAE7,12)和升高5-HT濃度較慢的缺點8,13,因此sertraline較適合用於MDD短期、長期治療,較不適用於急性期和復發時。
根據SCE試驗和SERT占用理論得知,SERT Occupancy須達80%才有足夠抗鬱反應13,15,但劑量超過治療閾值後(20ng/mL),抗鬱反應率卻沒有顯著正相關15,或許SCE和AR之間的關聯是遵循漸近函數(nearly asymptotic),即濃度低於治療閾值AR較差,反之高於治療閾值則AR穩定15,因此增加劑量可能無法取得更好的反應率和症狀緩解。但因樣本數太小仍有侷限性,不能斷言高劑量escitalopram療效和10mg相差無幾,目前臨床試驗對escitalopram 10mg的療效和安全性有充分證據,但20mg以上的escitalopram治療尚需更多的研究。
伍、 結論
綜上,escitalopram是SSRIs治療MDD病人在急性期、復發和短期的優先選擇,相對於其它SSRIs來說,副作用較輕,加上避免多頻次給藥,使得服藥順從性也較佳,降低造成療程中斷的停藥症候群風險。目前臨床試驗支持escitalopram 10mg有足夠的樣本數和對照組說明它的療效和低副作用,但在20mg或是更高劑量的escitalopram或24週以上的長期治療則尚未有更明確的用藥指引。給予escitalopram 10mg有治療效益,給予escitalopram 20mg以上劑量能否有更高效益或只相當於治療閾值的效益,仍持保留態度,目前臨床試驗不夠多,期待將來更多的臨床研究及文獻發表進一步整理、分析比較SCE高低濃度對AR上的差異和長期治療優劣點。
身為藥師須對治療MDD的SSRIs藥物有基本認知,包含藥物特性、頻次、常見副作用,扮演好專業藥師的角色、主動衛教SSRIs相關的不良反應和提醒切勿自行停藥,避免延誤治療時機,提升MDD病人用藥療效效益。
A Review of Escitalopram for Treating Major Depressive Disorder
Jia-Jie Ou1,2, Chan-Hseuh Lin1,2, Wei-Der
Lee1,2, Yu-Ying Chu1,2,
Yung-Hung Hsieh1,3
1Department of Pharmacy, Kuang Tien General
Hospital
2Taichung City New Pharmacist Association
3Hungkuang University
Abstract
Selective serotonin reuptake inhibitors (SSRIs) gradually became the main treatment for major depressive disorder (MDD). Overall, SSRIs has little difference in effects, but in the characteristics of drugs, the speed of effects and common side effects are different obviously. The common problem in the early stage of treatment is that the side effects may appear earlier than the effects. Patients will think that the drug is ineffective and the symptoms worsen, and they stop the drugs by themselves, causing a risk of discontinuation syndrome.
Because escitalopram not only acts on the primary site of serotonin transporter (SERT), but also acts on the allosteric site to facilitate the binding of escitalopram in the primary site, strengthen the effect of elevating the concentration of serotonin (5-HT) to increase the remission rate. The higher specificity of escitalopram also reduces side effects and has mild symptoms. It is taken escitalopram as the first choice in SSRIs for patients with MDD reasonably. In addition, the literature found that escitalopram uses a dose of 10mg or more, and its serum concentration of escitalopram (SCE) reaches the treatment threshold (20ng/mL). There is no significant positive correlation between SCE and antidepressant response (AR), but more and more trials and literature are needed to prove this association to further understand the therapeutic effect of high-dose escitalopram in patients with MDD at present.
參考資料:
1. American Psychiatric Association﹕Diagnostic and Statistical Manual of Mental Disorders, 5th ed. American Psychiatric Association, 2013.
2. Theo Vos, Christine Allen, Megha Arora, et al:Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015 Aug 22;386(9995):743-800.
3. Ronald C. Kessler, Evelyn J. Bromet ﹕The epidemiology of depression across cultures. Annu Rev Public Health. 2013;34:119-138.
4. 台大醫學院附設醫院精神醫學部﹕認識憂鬱 面對憂鬱 擺脫憂鬱。第一版。台北:衛生福利部,2015﹔6。
5. Christian Otte, Stefan M. Gold, Brenda W. Penninx, et al:Major depressive disorder. Nature Reviews Disease Primers. 2016 Sep;15.
6. Haiyan Li, Xinni Luo, Xiaoyin Ke, et al:Major depressive disorder and suicide risk among adult outpatients at several general hospitals in a Chinese Han population. PLoS One2017;12(10):e0186143.
7. 藥品仿單:Lexapro立普能®仿單, Apo-Citalopram安保喜樂®仿單, Zoloft樂復得®仿單, Seroxat克憂果®仿單, Prozac百憂解®仿單, Luvox無鬱寧®仿單。
8. Vaya Lalit, Prakash M. Appaya, Rajendra P. Hegde , et al:Escitalopram versus citalopram and sertraline: a double-blind controlled, multi-centric trial in Indian patients with unipolar major depression. Indian J Psychiatry. 2004;46(4):333-341.
9. P Favré﹕Clinical efficacy and achievement of a complete remission in depression: increasing interest in treatment with escitalopram. Encephale. 2012 Feb; 38(1):86-96.
10. Tianmei Si, Gang Wang, Fude Yang, et al:Efficacy and safety of escitalopram in treatment of severe depression in Chinese population. Metab Brain Dis. 2017 Jun;32(3):891-901.
11. Cipriani A, Furukawa TA, Salanti G, et al:Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. 2009 Feb; 373(9665):746-758.
12. Andrea Cipriani, Teresa La Ferla, Toshi A Furukawa, et al:Sertraline versus other antidepressive agents for depression. Cochrane Database Syst Rev. 2010 ;(4):CD006117.
13. Connie Sanchez, Elin H. Reines, Stuart A. Montgomery﹕A comparative review of escitalopram, paroxetine, and sertraline: are they all alike? Int Clin Psychopharmacol. 2014 Jul; 29(4):185-196.
14. Zhong H, Haddjeri N, Sanchez C , et al:Escitalopram, an antidepressant with an allosteric effect at the serotonin transporter - a review of current understanding of its mechanism of action. Psychopharmacology (Berl). 2012 Jan 219(1):1-13.
15. Vincenzo Florio, Stefano Porcelli, Alois Saria, et al ﹕Escitalopram plasma levels and antidepressant response. European Neuropsychopharmacology. 2017Sep; 27 (9):940-944.
通訊作者:歐佳傑/通訊地址:台中市梧棲區興農里興農路127-18號
服務單位:光田綜合醫院藥劑部/聯絡電話:(O) 04-26630936

